This study aimed to explore the educational needs of tuberculosis patients, based on their experiences in Karachi, Pakistan. Moreover, this study aimed to understand the challenges that the TB patients face in managing their disease. This research study was guided by a qualitative exploratory descriptive design. The purposive sampling technique was used to recruit participants for the study, and a total of ten TB patients was recruited from two TB treatment and diagnostic centers. The data were collected through face-to-face, semi-structured in-depth interviews. Data analysis for the study was done manually by following the five steps of content analysis, as discussed by Creswell (2013). Two major categories and associated sub-categories emerged from the analysis of the participants' narratives. The first category comprises perceptions and misperceptions of TB patients about their disease process, in terms of signs and symptoms, causes and spread, complications, and its treatment. The second category discusses the impact of TB on patients' lives; the financial hardships and the challenges faced by TB patients, such as those related to physical, psycho-social, sexual, and marital life. Tuberculosis (TB) is a major public health issue globally, and Pakistan is included in high TB burden countries. This study highlights that educational needs for TB patients are very important. The burden of TB can be reduced in Pakistan, and the care of TB patients can be improved through effective training of health care professionals. Moreover, further research and awareness programs at different levels can play a pivotal role in controlling and reducing the spread of this disease.
Tuberculosis (TB) is a major public health issue, as it has reemerged and is the second leading cause of death among infectious diseases worldwide (Knechel, 2009). According to Javaid (2011), TB is one of the ancient diseases and has been known for the last 5000 years, yet it is still affecting one third of the world's population and remains a major health problem globally. According to WHO (2009), 22 high burden TB countries, including Pakistan, account for 80 percent of the total global TB cases. The African regions have the highest incidence rate, whereas Bangladesh, India, Indonesia, China, and Pakistan together account for 50 percent of the global TB burden, while China and India account for approximately 40 percent of the world's TB cases. Pakistan is considered to be a high TB burden country.
Several researches have been done worldwide to assess the TB awareness level in TB patients and in the general public. The aim of one of the qualitative studies conducted in Malaysia, by Rundi (2010), was to assess the knowledge and perceptions of TB patients, their health seeking behavior, and the impact of TB in patients and their families. The interviews revealed that, the respondents did not know the cause of TB, and believed that TB occurred due to sharing of utensils or breathing space with TB patients, or eating contaminated food. The study participants perceived TB as a stigma-bearing disease that affects the financial, psychological, and physical aspects of their lives and life practices.
Financial constraints affect health seeking behaviors of TB patients in China; especially old aged and female patients were more reluctant to seek health care facilities and tended to visit basic health care centers rather than to go to general hospitals, as a majority of TB patient could not afford the cost of treatment, even though subsidized services were provided (Xu et al., 2004).
According to a study in Uganda, TB was viewed as a contagious disease; people believed that TB could be caused by sharing utensils with a TB patient, hard work, smoking, bewitchment, and hereditary transmission. Furthermore, some respondents mentioned that poverty affected treatment completion, while some reported TB as a stigma, but more as a stigma when accompanied by HIV co-infection (Buregyeya et al., 2011).
Several research studies have reported lack of knowledge, attitude, and practices regarding TB (Marks, Deluca, & Walton, 2008; Khan et al., 2006; Tasnim et al., 2012; Gilani & Khurram, 2012; Rundi, 2010; Ali et al., 2003). The WHO (2006) report reveals that, lack of knowledge and stigma about TB has negative consequences with regard to the use of available resources, delay in health seeking behaviors, and poor TB treatment compliance(Mushtaq et al., 2011).
The majority of studies have been conducted (Lu, et al. 2009; Safdar et al., 2011; Safdar et al., 2010; Tasnim, Rahman, & Hoque, 2012) on general awareness about TB. A study was conducted in two districts of Punjab, Pakistan by Mushtaq et al. (2011) to investigate the inequities in knowledge, attitude, and practices about TB among the urban and rural populations. The findings revealed that, the participants had poor knowledge regarding all aspects of TB, particularly in the rural populations. Health seeking behaviors were better in urban populations, as compared to rural areas, and almost half of the participants considered TB as a stigmatized disease. In their study, Khan et al. (2006) highlighted a significant fact that, in Pakistan more than 50 percent of the TB patients first visited a general practitioner in the private sector and, out of these, 10 percent delayed seeking treatment for more than six months after the onset of disease.
The reason behind the growing burden of disease in Pakistan is the delayed presentation of TB. Moreover, people have very limited knowledge about TB and its management, in general; this might be due to deficiencies in the National TB Control Program and lack of provision of proper health education by health care professionals (Javaid, 2011). Moreover, in Pakistan, owing to widespread misconceptions regarding TB patients, TB victims have a fear of social isolation such as stigmatization by society, and, hence, are reluctant in seeking treatment. This could be because of lack of knowledge and misconceptions related to TB which are extensive in Pakistani patients. These factors turn TB into a social stigma(Khan et al., 2006).
In Pakistan, a majority of the studies have highlighted poor TB awareness among TB patients and the general public; however, there are a few community based studies that have assessed the knowledge about TB (Ali et al., 2003; Gilani & Khuram, 2012; Khan et al., 2006; Mushtaq et al., 2011). Moreover, it is difficult to understand the experiences of TB patients owing to shortage of published studies.
The overall synthesis of all the studies indicates that, awareness about TB is not only poor in TB patients but in the general public as well. The increasing cases of mortality and morbidity due to TB in high burden countries, including Pakistan, have become a significant health threat and a challenge to the health system. It is important to mention that, in most of the studies discussed above, with respect to other countries, there is a dearth of qualitative research studies that have explored the knowledge of TB patients and the challenges they are facing. The same is the case in Pakistan. Hence, for exploring the educational needs of TB patients and identifying their problems in Pakistan, it was worth conducting a qualitative research study to explore and identify the educational needs of TB patients, based on their experiences and challenges.
This research study was guided by a qualitative exploratory descriptive design. The sample size in qualitative research is determined by the informational needs of the phenomenon under study and the actual sample size is decided upon the saturation of data. So, a total of ten patients were recruited for this study and the principle of data saturation was applied, while determining the sample size. The purposive sampling technique was used to recruit the participants for this study, as it is considered to be the best strategy, in which the participants that best contribute to the information needs of the study (Creswell, 2013) are selected. The eligibility criteria for participation in this study included:
(a) Patients with active TB who had been under treatment for at least six months,
(b) aged 18 years and above,
(c) Participants who were willing to participate in the study,
(d) Patients who were not at a contagious stage.
Data was collected from March 2014 to May 2014. Face to face, semi-structured, in-depth interviews were conducted for the collection of data, as these ensure that, the investigators obtain all the information required. All interviews, which lasted for about 20-40 minutes, were audio tape recorded. It was ensured that, interviews were conducted according to the time and day feasible for the participants. Prior to the interviews, the participants were always asked whether they had any issues or concerns regarding the interview. A self-developed semi-structured interview guide was used to conduct the interviews. Keeping in view the participants' comfort level, all interviews were conducted in the Urdu language. Field notes were also taken to capture the participants' actions, which could not be covered through audio tapes. These notes helped in describing the participants' emotions and gestures.
For data analysis, content analysis was done. The tape recorded interviews were transcribed into Urdu and then translated into English. Data analysis was started side by side with data collection, so that further questions could be added in the interview guide, where needed and unclear questions could be clarified from the participants (Creswell, 2013). The process of data analysis was guided by the steps given by Creswell (2013). Inductive coding was used to analyze the data by using the latent and manifest approach of content analysis; similar codes were assigned a category and sub category, and then categories were developed with associated sub categories.
The interviews were conducted in Urdu and then translated to English for analysis. So, to depict the true essence of the feelings of the study participants, some parts of the Urdu narration are shown in brackets, besides their English translation. Moreover, since in this study, some of the participants were in the recovery phase from TB while others were on a continuous TB treatment course, therefore, the language of the narratives is in both the present and the past tense.
The study approval was taken from the Ethical Review Committee (ERC) of Aga Khan University, Karachi, Pakistan. Prior to involving the participants in the study, informed consent was taken by informing each participant about the research title, the purpose of the study, benefits and risks, and their rights regarding participation. The participation in the study was on a voluntary basis and participants were assured that, they could withdraw from the study at any time.
Confidentiality and anonymity of the participants were maintained during and after the study by assigning codes. The safety of data was ensured by keeping hard data locked and soft data password protected. The raw data could only be accessed by the researcher. To maintain trustworthiness in this study, the Lincoln and Guba (1985) criteria were followed, which include credibility, conformability, dependability, and transferability.
A total of ten TB patients participated in this study. Out of a total of ten, there were seven male and three female participants, most of whom were married. Their age ranged from 18 to 60 years, the average age being 39 years. In terms of their education, four were illiterate, while the rest of them had a primary or secondary level of education as shown in Table 1.
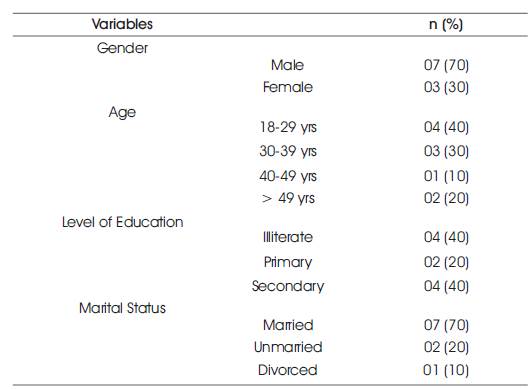
Table 1. Demographic Profile of the selected TB patients
Half of the participants had been suffering from the disease for more than one year, while the other half for less than one year. None of the ten patients had ever received formal or informal education on TB. With regards to having knowledge about the disease, four had received information from health care professionals, whereas, six participants expressed personal experiences/perceptions shown in Table 2.
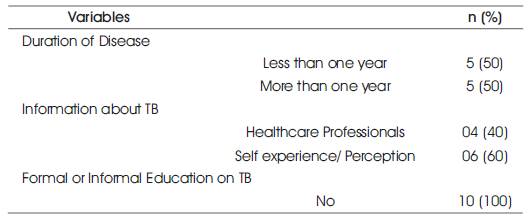
Table 2. Patients' Disease Information
The analysis of the narratives led to two categories and associated sub-categories, as shown in Table 3.
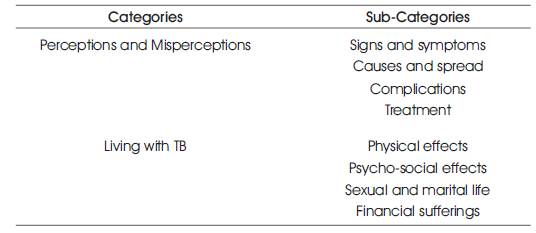
Table 3. Categories and Sub-Categories
This category comprises of the participants' perceptions and misperceptions about the signs and symptoms of the disease, its causes and spread, complications, and treatment.
Most of the patients reported that sputum with cough, weight loss, loss of appetite, chest pain, hemoptysis, and fever occurred along with cough, in TB; in addition, some misperceptions also existed, such as loose motion, vomiting, and kidney problem. All of the participants viewed chronic/severe cough as one of the most common symptoms of TB. As one patient expressed, “Cough that persists for a long time, I mean an old cough, that is one of the most common signs” (PM 01). Another participant, who was about to complete his TB treatment expressed:
“I have experienced and heard about TB that one suffers from cough for a long period, consistent cough for two to three weeks, sputum production, on and off fever, loss of appetite, weight loss; all these are symptoms of TB” (PM 04).
Several of them reported chest pain that resulted from coughing; some of them explained the nature of cough and the pain; as one of the patients who had a relapse of TB stated:
“Whenever, I cough, blood comes out from my mouth. I have cough that is blood stained, and there is severe pain in my ribs. Sometimes I also have pain in this place [referring to the posterior side of chest]. The pain is so extreme that it makes me scream” (PF 09).
Although, a few participants knew about the exact signs and symptoms of TB, they expressed their views with some misperceptions based on what they experienced during the course of their disease. As one of the patients stated, “When I was diagnosed with this disease [TB], I had vomiting and loose motions at the beginning of this disease” (PF 06). Similarly, one of the patients, sharing his experiences, stated, “It [TB] is like, you will have high grade fever, which will never subside, and you have severe vomiting… and you do not feel like eating anything. If you eat, you would vomit instantly….” (PM 03).
Close contact with a TB patient, germs, spitting of sputum, and sharing utensils with TB patients were identified as a means of spread and causes of TB. However, some of the participants also reported, misperceptions related to the cause of this disease, such as the notion that TB is caused by sharing clothes with TB patients, or having their leftover food, and also having intercourse with them. Some also believed that, it is an inherited condition. Tobacco use was also seen as one of the causes of TB. Thus, participants expressed different perceptions about the cause and spread of TB. Most of the patients were able to point out accurately that, TB is a communicable disease, and it spreads from close interaction with TB patients. As one of the patients said:
“It is like, for example if I am a patient of TB, the disease can be transmitted to others from me. It [TB] is a communicable disease. If you [referring to a TB patient] eat together, drink together, and sit together with other people, it [TB] can spread to them” (PM 05).
One of the patients communicated, “Others can get this disease [TB] through sitting together, eating, and drinking” (PM 10). Another patient, who expressed his perception by giving an example and sharing the germs theory, asserted:
“If you [referring to a TB patient] sit close to a person and talk to him, the other person would get it [TB]. Obviously, if you exhale after cigarette smoking, then you will see it in the form of smoke, but when you exhale in respiration, no one sees. Similarly, when you inhale air and then when you exhale, the germs spread in the air” (PM 01).
Half of the participants associated positive family history as a cause of TB, and expressed that it is a familial disease, which runs in the family. One patient stated, “This disease [TB] is hereditary that is present in our family. My niece and her mother also have TB. So, this disease runs in families” (PF 08).
Some of the participants related the cause of this disease with Tobacco and Betel nuts; as one patient expressed, “It may be caused due to excessive consumption of “Gutka” and Tobacco; obviously, there must be some side effects of these things, and one of them is this disease [TB]” (PM 07).
Most of the participants identified several measures to control the spread of this disease. One participant said:
“You should take precautions. Wear a mask, and stay away from children while you have this disease. Take safety measures, be careful, especially while eating or drinking, do not eat waste food, and keep wearing a mask. Maintain a distance while talking to people. Stay at a distance while talking to someone” (PM 03).
A participant, who had a relapse of TB asserted that, “We [referring to TB patients] should take precautions, that we do not use anything which is being used by other people….” (PM 07).
Similarly, another participant stated:
“You [referring to a TB patient] may use a mask, as it protects you from the dust and others from the air you exhale. And the sputum should be spat out at a place where it canbe drained easily, such as sink; and if you spit in an open space, then you should make sure that people are not sitting around that place” (PM 01).
With regard to complications of this disease, the majority of the participants shared almost the same concerns that in TB there is a risk of death and lifelong suffering. As one participant commented:
“There are a lot of consequences. It [TB] is a biggest threat to one's own life. This disease may also spread to others, and your family is at risk from you. If a person expires, it is a loss for the family members” (PM 07).
Another patient expressed, “If you [referring to a TB patient] do not treat it [TB], you keep falling sick. We [referring to TB patients] will be bed ridden, and will have backache. You can lose your life, if you do not treat it, and do not take precautions” (PF 06).
One of the female participants had fear of death and stated, “If you do not treat TB, you can die. I am more scared of death, if I do not take medications, my lungs will be destroyed” (PF 08).
Some of them not only expressed their fear of death, but also fear of being abandoned by their family members. As one of the patients articulated, “As the disease aggravates, your suffering becomes intolerable and the chances of death increase. Due to constant cough, the person is unable to sit in the company of others who are likely to feel threatened and, hence, avoid your company” (PM 01).
Several participants had correct knowledge about the treatment of TB. However, only a few of them discussed the DOTs centers, and the majority of them were only aware of the center, where they were getting their treatment. They were either told about it by their friends or they had had their family members treated from the same place. One of the patients shared, “There is a treatment available for this disease [TB]. So, we should not lose hope; this is a wrong perception that there is no treatment for TB. Poor people can obtain treatment at these centers (DOTs centers)” (PM 02).
Most of the participants were aware that, the duration of the treatment varied according to the progression of the disease, and they also insisted on precautions. As one of the participants stated:
“The first treatment of TB is taking precautions. Then, its treatment depends upon the kind of courses of TB drugs, such as a six month, or a nine month course. It also depends on what stage of TB a person has reached” (PM 01).
Some of the participants stressed on the regularity of the treatment to prevent a relapse of this disease, which required a strong will power. As one of the patients shared, “Whatever medicines the doctor has recommended me, I use them regularly, without any break. I have been taking treatment for almost six months from this place” (PM 04). Another participant stated, “It is just that you [referring to a TB patient] have to treat it with determination. “InshAllah”, it [TB] will be cured” (PM 03).
Several patients highlighted the longevity of treatment for TB. For the effectiveness of treatment, they also stressed the importance of a good diet, especially that one rich in protein, and also on the value of rest along with medication. One of the patients shared her perceptions by saying, “They [health care professionals] said it is a nine month course, requiring medicines with rest. However, the recovery largely depends on the diet, which should be meat, and fish, as compared to medications”(PF 08).
Patients living with TB reported significant challenges that were not limited to the physical affects only, but also affected their psycho-social conditions, sexual and marital affairs, and also financial status.
With regard to the physical effects, most of the participants experienced lack of appetite, breathlessness, vertigo, weakness, and weight loss that ultimately affected their daily activities, and also affected their ability to work, especially if the work was physically demanding. Consequently, their earning ability got compromised. One of the patients narrated his experiences by saying:
“I have become very weak. I mean I have lost weight… Obviously, due to it [TB], everything is affected. For example, if you [referring to a TB patient] were able to do any job requiring weight lifting, such as loading something, now, you will not be able to do that job after having this disease [TB]. I mean, it will take time to do it again” (PM 01).
A participant, who was anxious to earn for his family, stated, “I have lost weight, developed weakness and shortness of breath, and cannot do any work….” (PM 02). Likewise, another patient shared:
“There is no sensation in my body. I become breathless when I walk, andI have a burning sensation in my legs. I feel so drained out that I cannot do any work…. I experience sudden shortness of breath and have vertigo as I climb up and down the stairs” (PM 05).
Describing her experiences, one of the female participants who worked as a maid, explained the severity of her symptoms,“I experience vertigo so frequently that I have repeated blackouts. I have become very weak, so much so that, I have collapsed on the way many times while going to work. I even pass out while working” (PF 09). Similarly, another participant said, “My weight is 25 kg; It has decreased a lot…., and my skin complexion has also darkened. I cannot do any work, because I am very weak and get tired easily” (PF 08).
Most of the study participants expressed feelings of social isolation that they experienced due to their family members, relatives, friends, and people in social gatherings. Several patients felt fearful, ignored, stigmatized, and distanced from the society, which had negative psychological effects on their health. Most of the participants felt stigmatized, albeit, at varying levels. Based on the contagious nature of the disease, they were either abandoned by others, including friends and family members, or they isolated themselves from others. Although, some of them took voluntary precautions to prevent the disease from spreading to their family members, others did it due to the fear of rejection or being questioned.
Several participants felt that, they were being ignored; as one of the patient reflected:
“People have fear about the transmission of this disease [TB] to them. And secondly, a majority of them think that, it [TB] is a contagious disease [Chootkibeemari]. However, it is a germ that can be transmitted to you. I guess they are protecting themselves by keeping a distance from you” (PM 01).
Likewise, a participant, who was the eldest member and the sole bread earner of his family, shared his experience of being ignored, and stated:
“If someone knows that you have TB, then they avoid you. They will hesitate in their interaction with you. One of my relatives did this with me, so now I really take precautions while eating with him. Thank God, that my family members did not do it, because, obviously, they are living with me…. I am the eldest in the family, but I can tell if someone keeps a distance from me, though they do not show it apparently. I myself take precautions, and so they feel it” (PM 07).
The above excerpt indicates that, people may not openly tell you about taking precautions, if you have authority over them by age or you have a good social standing.
A female participant, who was sent back to her parents' home shared:
“I do not visit people as I fear that, they might say why are you eating in my plate, then….? My own sister-in-law separated my utensils, while my husband has kept me here because of this disease [TB]; he will take me once I recover” (PM 08).
Some of the participants took precautions either to prevent its spread to others or due to fear of rejection. As one of the patients elaborated:
“It [TB] has absolutely affected my life, and I myself avoid meeting with people. When the disease [TB] began, I did not even sit with my friends, and stayed more at home. And I went only for my work. So, my routine was to go for duty, and then stay at home” (PM 03).
Likewise, one of the male participants limited himself to his room and did not want to go anywhere in order to avoid facing people's questions about his disease. He marked, “I do not want to go anywhere…., and I just keep sitting at one place, because people will ask about my disease [TB] and condition. That is why, I do not go anywhere” (PM 10).
The female participants have different experiences, as one of the female participants who was divorced, had not disclosed her disease to others. She asserted,“I did not disclose my disease to anyone…. People do not let you live, this world is bad. No one likes to meet you [referring to a TB patient]; nobody likes to come and to talk to you, and I fear that, nobody will come to my home if they find out” (PF 06).
Most of the participants indicated that, their sexual and marital life was affected because of TB. Some of the participants expressed that, due to the fear of TB transmission, they stayed away from their spouses. The female patients' lives were badly affected by this disease, as one was divorced and two were separated after their diagnosis of TB. The researcher noted that, during their interviews, usually, the male participants avoided describing the effect of their disease on their marital life. Some of them refused to comment when probed directly by the interviewer.
One of the male patients, who was scared of transmitting TB to his wife, expressed:
“At that time it [referring to marital life] was affected, because I myself was not physically strong. When a person is physically strong, then everything is normal. Secondly, I knew that, if I did not take precautions, then this disease [TB] will transfer to her [his wife]” (PM 01).
Another participant commenting on the effect of TB on his marital life, said:
“Nothing happened, we slept together in one room, but I did not have sexual contact with my wife, as I was weak, and was also in stress. I coughed continuously, so, it was disturbing. But, sometimes, when the cough was severe, I used to sleep in a separate room” (PM 02).
Participants who were single, had different views, and completely denied TB implications on their sexual health; as one of the patients articulated, “Sexual life was not affected that much…. That is all I want to say about it. It was the same as before. There is no such problem in that [sexual health]” (PM 03). Likewise, another stated, “No, it has not affected me that much but there is a lot of weakness” (PM 10).
The female participants had different perspectives, and reported misperceptions as well. One of the separated female patient perceived that, extra marital sexual contact was one of the main causes of TB. She reported, “Sexual life has spoiled my body. I have got this disease [TB] because my husband has contacts with other women, so he transmitted this disease to me. It [sexual relationship] is the main cause of my disease [TB]” (PF 08).
Another participant stated, “I am living with my mother after I was diagnosed with this disease [TB] and my husband avoids me. He does not come close to me. He says when I recover, he will take me home” (PF 09). Another female participant, who was divorced, shared that she was fine and had recovered from the disease. She commented:
“Thank God, I have recovered a lot after the treatment. People who see me they tell me that I look good again. It [TB] has not affected that (Sexual health), in fact, it has improved, thank God…. If I get married, I will have tests done to check whether I still have TB or not” (PF 06).
Financial sufferings. As discussed earlier, most of the participants were worried about their finances due to compromised physical health, as they were unable to work and earn money. Since all the participants belonged to the low and middle socio-economic class, most of them had physically strenuous jobs; thus, they were also financially affected by TB. Their expenses had also increased, and so, their financial condition was badly affected by this disease. Though a majority of the participants had started their treatment from private practitioners, owing to problems faced by them due to lack of financial resources and expensive treatment, they were referred to the DOTs centers either by their friends or relatives. Although, the treatment was free of cost here, they were unable to manage their finances. One of the participants, sharing his worries, said:
“It has been six months since I had this problem [TB], and I have left my job. Now, I cannot do any work, so I have no income. This disease [TB] has severely affected my financial condition. I used to do double duty, but now I cannot even do a single job. I pray to Allah that I may become healthy again and start double duties, because I am unable to make both the ends meet” (PM 02).
A few participants shared their financial worries regarding the diet prescribed in this disease. As one of the patients, who was a student, articulated that:
“My monthly stipend is 1000 rupees, and before this disease, it was enough for my expenses. Now, as I use medications, 1000 rupees are not enough for even 10 days. I can hardly make my both ends meet. Treatment is free of cost, but I was advised by the doctor to take milk, juices, carrots, bananas, apples, fish, and chicken. Who can afford to eat all these things in only 1000 rupees?” (PM 10).
The female participants faced almost the same difficulties while managing their finances, as they belonged to the low socio-economic strata, and were managing their expenses on their own. One of the participants shared:
“Our circumstances have worsened. Doctors say eat fish, egg, and take milk when you have TB. But for me, it is even difficult to have a decent meal on time…. I do not have a permanent job, I just clean people's houses, and they give me some money, which is not enough to survive” (PF 08).
The findings of the present study revealed that, most of the participants had good knowledge about the signs and symptoms of TB; specifically about the nature of a cough that was identified as the most common symptom of this disease. This finding corresponds with the findings of other studies (Ali et al., 2003; Anjum, Daud, & Mukhtar, 2009; Das, Basu, Sinjita, & Das, 2012; Khuwaja, & Mobeen, 2005; Lu et al., 2009; Mushtaq et al., 2011; Tasnim et al., 2012) that reported cough as one of the most common symptoms of this disease.
Participants showed a good understanding about the signs and symptoms of TB, and most of the study participants were aware of some of the common symptoms of this disease. This finding is similar to the findings of the studies in Pakistan and other countries in the region (Anjum, Daud, & Mukhtar, 2009; Buregyeya et al., 2011), which revealed that, a majority of the participants identified cough persisting for more than three weeks, fever, hemoptysis, weight loss, shortness of breath, and cough with blood as the common symptoms of TB.
According to most of the study participants, sharing utensils and close contact with the affected people were the main sources that caused and spread this disease. Likewise, (Anjum et al., 2009; Buregyeya et al., 2011; Rundi, 2010; Zhang, Liu, Bromley, & Tang, 2007) reported that, majority of the respondents had expressed that, it can be caused and spread by sharing of food and utensils and close contact with the people affected.
With regard to controlling the spread of TB, the study participants asserted that, it is advisable to take precautions, and avoid close contact and sharing of utensils with other people. Similar findings were reported by Mushtaq et al. (2011) whose study participants identified almost all of the precautions stressed upon by the participants of this study.
In line with the existing literature (Khuwaja & Mobeen, 2005; Sharma et al., 2007), most of the participants in the current study showed good awareness about the consequences of not treating the disease; they knew that if not treated, it could lead to the worsening of the condition, could become a potential risk to others, and, in extreme cases, could also lead to death. Consistent with existing literature (Ali et al., 2003; Buregyeya et al., 2011; Gilani & Khurram, 2012; Ottmani, Obermeyer, Bencheikh, & Mahjour's, 2008; Sharma et al., 2007), most of the patients in the current study showed good knowledge about the treatment regimen of TB.
In a study, Karim et al. (2011) and Rundi (2010) reported that, the patients showed concerns about loss of employment, and inability to handle a heavy work load due to the physical effects of TB on their health, which obviously affected their earning capacity as well. Similarly, most of the patients in the current study shared the same concerns.
The findings of the current study revealed that, a few participants received support from family members, relatives, or friends, when they were diagnosed with TB. This finding is similar to that of Long, Johansson, Diwan, and Winkvist's (2001). However, as reported in previous studies, by Karim et al. (2011) and Khan et al. (2006), in the present study, the female participant who was divorced had kept her disease undisclosed, and two female patients were forced to go to their parents' house during the course of their disease.
In line with the existing literature (Karim et al., 2011; Xu et al., 2004), a majority of the participants in the present study reported that, becoming victims of social discrimination, and also felt that, the society tried to avoid and ignore them. Zhang et al. (2007) noted that, a majority of unmarried participants reported that, they were likely to have difficulty in finding a life partner for themselves, as they had TB, which is considered as a stigmatized disease. The findings of the current study revealed that, unmarried participants denied any impact of TB on their sexual health; this might be due to the stigma related with TB, and also due to masculine ego.
Most of the patients in the current study perceived that, TB had badly affected their financial condition, even though the treatment was free of cost. These findings coincide with those of the previous studies (Karim et al., 2011; Liefooghe et al., 1995; Long et al., 2001).
A study conducted in Morocco by Ottmani et al. (2008) reported that, 85 percent of the respondents did not receive any information about TB for the health care services. In the present study, it was disappointing to see that, none of the study participant had ever received formal or informal education related to TB.
Several studies (Ali et al., 2003; Buregyeya et al., 2011; Liefooghe, Michiels, Habib, Moran, & De Muynck, 1995; Mushtaq et al., 2011; Nnoaham et al., 2006; Ottmani et al., 2008; Zhang et al., 2007) have reported that, TB was perceived as a stigmatized disease, that TB patients are usually rejected by the society, and those patients restricted their social mingling to minimize facing the possible stigmatization associated with TB. Patients in the current study reported a profound social impact and expressed that, they preferred social isolation and avoided social gatherings, and distanced themselves from people due to the stigma related to TB. The current study also indicated that, the female patients were affected more when compared to the men.
In the light of the study findings, the healthcare professionals should have sound knowledge about TB and must inform the public that, TB is a curable disease. They should take measures to clarify the misconceptions and dispel myths about TB in order to eliminate the stigma associated with this disease. The government agencies and non-governmental organizations need to allocate funds for TB patients, particularly for those who are underprivileged and unemployed, to ensure regular treatment and to minimize their financial burdens. These measures would ensure disease prevention and health promotion in the country.
The findings of the study revealed that, the patients have basic knowledge about the disease process; however, misperceptions also exist regarding the causes and transmission of this disease. Moreover, TB has a negative impact on their lives in terms of physical, psycho-social, sexual, and financial sufferings. The findings of this study and the reviewed literature revealed that, TB patients of both developed and developing countries have similar perceptions about the disease, and its effects. Recommendations provided in this study may help in raising awareness, improving care, and controlling the incidence of TB in the country.
Pakistan ranks high amongst the countries with the highest prevalence rate of TB in the world. Therefore, there is a need to explore the problem further in order to reduce the burden of the disease in the country and, thereby, also help towards achieving the MDGs. Moreover, gender perspective studies need to be conducted to understand gender differences between men and women suffering from this disease.