This paper assess the effectiveness of Hoku point massage with ice on the severity of venipuncture pain in children with thalassemia. This was a double-blind, two-group clinical trial. Eighty six Thalassemic children who were eligible to participate in the study were selected from children referring to Kerman Samen Alhojaj Medical Center consisted the study population. By using a convenience sampling method, they were placed into experimental (Hoku point massage with ice) and placebo (touching ice marble on fake point of the back of the hand) groups by random allocation. Data was collected using a questionnaire about the child's demographic information and FLACC (Faces, Legs Activity Cry Consolability) behavioral pain scale. Descriptive and analytical statistics using software SPSS v. 22 were used to analyze the data. Finally, the results show that average pain score in the experimental and placebo groups was 0.65 ± 0.75 and 2.56 ± 1.58 respectively. There was a statistically significant difference between these two groups in terms of pain severity (p = 0.0001). According to the results, ice massage at Hoko point is an effective method to relieve the venipuncture pain in children with thalassemia.
Thalassemia is the most common hereditary blood disorder and approximately 240 million people worldwide carry beta thalassemia [1] . Approximately 2,00,000 patients with thalassemia major have been documented in the world and each year about 60 million people will be added to this figure [2]. Thalassemia is the most common genetic disease in Iran. In Iran, about 3 million people are carriers of this disease, and about 26,000 people have thalassemia major and about 800 people are added to this figure annually. Major beta thalassemia is treated by blood transfusion [3]. Placing venous catheter is the most common invasive procedure which may cause pain in children. Pain caused by invasive procedures such as venipuncture causes physical and psychological stress in children. Pain resulted from penetrating needles or catheters into blood vessels are problematic when they must be used repeatedly. Since venipuncture is considered a preservative treatment in children with thalassemia, nurses must try to minimize discomfort for children. To achieve this goal, several pharmacological and non-pharmacological methods have been proposed; of them, non-pharmacological or independent methods are considered as desirable and useful strategies to improve children's experience of painful procedures [4]. Ice massage is one of these non-pharmacological treatments. Hoku point (LI4) used in this study is located in the middle of the angle between the first and second bones of the palm, between the thumb and the index finger on the back of the hand. This point is the most important numbness point whose stimulation alleviates pain in the body [5]. Researchers think that, the effect of ice massage results from involvement of the pain gate control system. Indeed, when the impulses caused by shaking, scratching and ice massage reach the posterior horn of the spinal cord, they act like a valve and guide pain to the higher brain centers and thus alleviate pain [6]. Using acupressure at point UB32, Suhrabi et al (2014) were able to reduce the pain of intramuscular injection [7]. Yesmail et al (2012) also found out that, ice massage of Hoku point, as one of the safe and non- pharmacological methods, was effective in reducing labor pain [8]. Concerning the fact that alleviating pain in children is part of their rights and since this emotional pain and stress caused by increased injections may be one reason for the delay in venipuncture, which is essential for nurses to take any action appropriate to relieve pain. Concerning the importance of the subject and since no studies have been recorded in this area in Iran [9]. This study ,thus conducted to investigate the effect of ice massage of Hoku point and placebo on severity of venipuncture pain in children with thalassemia.
This clinical trial study was of double-blind, two-group type; patients were not aware of the group which they were in and researcher that measured severity of pain did not know about the aim of the study.
The study population was all school-age children referring to Kerman Samen Alhojaj Medical Center (Kerman is one of the biggest cities in Iran and is the center of Kerman province in the South East Iran. This city is the central part of Kerman ward and its population, according to the 2006 census by the Statistical Center of Iran is 5,15,114) [9]. Inclusion criteria included; the score of pain with Wong- Baker FACES Pain Rating Scale before venipuncture was zero, Thalassemic children aged 6-12, having a record in the center, being aware of the location, time, person, ability to have verbal communication and patient's willingness to participate in the study. However, children with physical problems (verbal, mental, visual and auditory), mental disorders, administering medication to reduce pain for up to 8 hours prior to venipuncture, penetration of more than one catheter into the skin, or prolonged duration of catheter insertion (over a minute). Neuropathic disorders resulted from diabetes; fractures and inflammation in the massage point as well as having any pain before venipuncture was excluded from the study. The sample size formula was:


Sample size was 40. Six extra samples were added to the sample size because of the possibility of attrition. Finally, 86 subjects were selected and allocated into two groups (ice massage at Hoku point) and placebo (touching ice on fake point of the back of the hand) by using stratified random allocation. 43 subjects were placed in each group.
After obtaining ethical code from Kerman medical sciences (k= 92/45) and permission from the Thalassemia Center, sampling was started. The researcher introduced herself to the participants and obtained written consent from the parents and verbal consent from the children.
Data was collected using a questionnaire about the child's demographic information (age, sex, age at diagnosis) and behavioral pain scale (FLACC). Behavioral pain scale consists of five parts: Face, Leg, Activity, Cry and Consolability. Each section has a score (0-2). Higher scores show more response to pain. The score of each section was written separately and then scores of all five sections were added to calculate the total score. Score range was from 0 (lowest) to 10 (highest) [10]. Stefan Nilson et al., (2007) introduced FLACC behavioral scale to assess pain procedures in children aged 5-16 [11].
Reliability and Validity were evaluated using the kappa test (k = 0.85, P <0.0001). In Iran, Sadeghi et al. has confirmed the content validity of this scale by 7 by the faculty members of the Qazvin Nursing University and for reliability they used it for 20 children and with a combined form of FACES its reliability was confirmed (r=0/7,p<0/001) [12]. In this study, content validity was confirmed by 10 teachers in the nursing field. And reliability confirmed by test retest and was (0/85).
Data was collected before and during a venipuncture. Child's demographic information was completed through interviews with the child or the child's relatives. Then, to determine the Hoku point, the child's thumb was placed in the abduction position; in this case, a muscular prominent peak (related to the thumb adductor) was the Hoku point. In the experimental group, some icy marbles (2 cm in diameter) were placed in plastic gloves and then were wrapped into one-layer cotton cloth. The researcher messaged the subject's hand (the hand that was not used for venipuncture) slowly and rotationally with icy marbles 5 minutes before penetrating IV (Researcher was trained by an expert in this regard). Each time, maximum pressure was for one minute, and massage was stopped for 10 seconds. This intervention lasted for 5 minutes. In the placebo group, the same method was used except that the icy marbles were placed on the fake point on the back of the hands without any pressure or massage [4] (the area between the third and fourth metacarpal bones) shown in Figure 1.
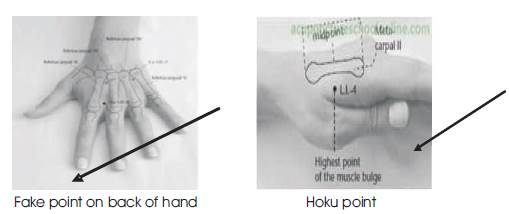
Figure 1. Points Used in the Test and Placebo Groups
Using FLACC behavioral scale, venipuncture pain scores were observed and recorded in both groups by the researcher assistant. The nurse in charge of venipuncture, IV size, type and manufacturing company, venipuncture place and conditions were all similar in all venipuncture. Venipuncture was successful on the first try and was not repeated. To have equal work for both groups, IV was done only by one skilled nurse in the thalassemia section from minimum distance of 5 cm from the vein at an angle of 30 to 45 degrees [13]. In this study, a single researcher did all experiments (ice massage and ice touch) for all the subjects so as to avoid any bias. The subjects were assured that, there was no known complication for their intervention and that they would be referred to the physicians in the case of problem. Before the intervention started, both groups were taught how to use a behavioral pain scale to express pain.
Data was analyzed by descriptive and analytic statistics using SPSS software version 22; the significance level was considered 0.05. The Shapiro-Wilk test showed that, the data were not normally distributed so non parametric tests were used to analyze the data. To compare the variables between two groups, Mann-Whitney test was used. To determine the relationship between variables, the Middle regression was used. Chi-square test for difference in both groups.
The findings of the present study showed that, 45.3% of subjects were girls. Chi-square test with a significance level of 0.83 showed no significant difference in both groups in terms of sex. Mean age was 9.49 ± 2.1 in ice massage and 9.88 ± 2.3 in the control group. Mann- Whitney statistical test showed no significant difference between children in both groups in terms of age (P= 0.99). Mean age at diagnosis was 9.2 ± 11.52 in the ice massage of Hoku point groups and 6.86 ± 5.79 in ice touch in the fake point of the back of the hand shown in Table 1. Mann-Whitney test showed no significant difference between both groups regarding age of diagnosis (P=0.57). Reviewing the relationship between pain and variables through Spearman correlation coefficient, it was shown that there was no significant relationship between pain and age (P=0.28) and pain and age at diagnosis (0.89). The Mann-Whitney test showed a significant difference between both groups in terms of severity of pain; that is, the mean pain score in the ice massage of the Hoku point group and ice touch on the fake point group was 0.65 and 2.56 respectively.

Table 1. Comparing the two groups of variables: age, age at diagnosis, and pain using Mann-Whitney test in Experimental group (1) and Placebo group (2)
Regression test showed that, demographic variables (age, age at diagnosis and sex) had no effect on pain score. Comparing pain scores between the experimental group and the placebo group, it was shown that, median pain score was more in ice touch group than in ice massage group (there is a significant difference between ice massage and ice touch groups) shown in Table 2.
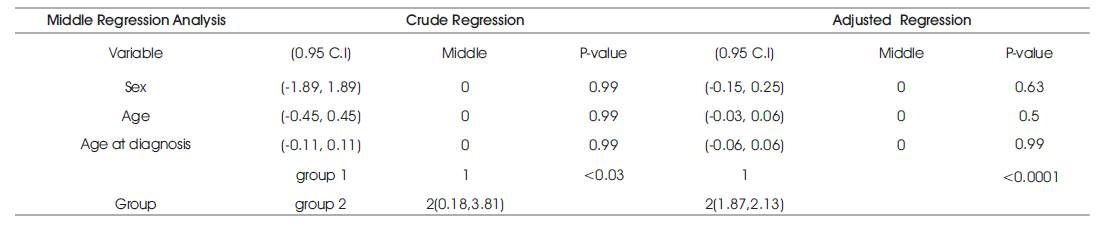
Table 2. Comparing pain scores between Experimental group (1) and Placebo group (2)
The results of this study showed that, ice massage of Hoku point, as one of the non-pharmacological methods, is effective in alleviating pain caused by venipuncture in children with thalassemia. Many studies have pointed to the effect of Hoku point massage with ice on relieving pain. Results of this study are in line with the results of [6], that they used acupressure and using ice massage to relieve pain and their results showed alleviate pain. [14] relieved pain caused by intramuscular injection (on point UB 31). There are other studies on the effect of ice massage of Hoku point for pain relief in cases other than injection. In their studies, Kaviani et al. (2011) and Haj iamini et al. (2012) used ice massage of Hoku point to reduce labor pain in pregnant women [15,16]. Also Hjelmstedt et al. (2010) concluded that, acupressure in SP6 point was effective in reducing pain in the labor active phase when other methods were not available [17]. Using ice massage of SP6 point, Rakhsh Khorshid et al. (2013) could reduce the severity and duration of dysmenorrhea pain[18]. Since both groups were similar in terms of different variables (gender, age, age at diagnosis), it can be said that difference in pain intensity was affected by none of the controllable variables in this study: it was one of the key findings in clinical trial research.
Results show that, there is a reverse relationship between pain and age (p=-0.02), but it is not significant statistically (p=0.83). In a study carried out by Borhani et al. (2010), no significant relationship was observed between the age and severity of venipuncture pain [4]. In a study by Alavi et al. (2008), no significant relationship was observed between age and severity of venipuncture pain [19]. In a study by Sparks, a touch reduced injection pain significantly, but had no significant relationship with the age and sex of the child [20]. In a study by Mazhari et al. (2008), pain severity was not significantly different in different age groups [21] . This result was in line with the results of studies conducted by Jeske et al [22] and Chambers et al [23].
Another finding of this study is that, there is no significant relationship between sex and pain (P=0.49). Although many studies indicate that, there is a relationship between pain and gender, there are other studies show that this relationship does not always exist. In their study, Myers et al. (2006) showed that, a significant relationship existed between boys and girls in response to pain [24]. It was shown in a study by Ayesh et al. (2007) that the pain threshold was equal in men and women [25]. Moreover, Bargon et al (2002) showed that, pain threshold was equal in men and women [26, 27]. Other studies have also shown that, response patterns of pain are different; for example, women complain more about the backache, while it is not obvious in men [28]. Also, a new study has shown that women, in vitro, report pain more significantly than men. However, when it comes to factors such as level of anxiety and stereotypes associated with the trends of report pain, results show that, sex is not a significant predictor in reporting pain; it is in line with the results of this study. However, one of the limitations of this study is that, pain reduction in the experimental group cannot be exclusively related to Hoku point massage with ice and that every acupressure may show such results.
Concerning the results of this research, it is suggested that, nurses and other members of the treatment team will use ice massage of Hoku point in children with chronic diseases who repeatedly undergo painful therapeutic procedures (e.g. thalassemia, cancer, etc.) so as to provide them with a less painful life and more natural growth and to improve quality of their lives. Concerning the important role of nurses in the health team, it is hoped that, the results of this research, as one of non-pharmacological methods of alleviating pain, can pave the way for nurses to do their duties better and can be used as a painless (or with lower pain) experience in venipuncture in children in thalassemia centers.
According to the results of this study, it is suggested that, the effects of acupressure on pain caused by invasive procedures in school age children with other chronic disease as well as before surgery and examined with a larger sample size.