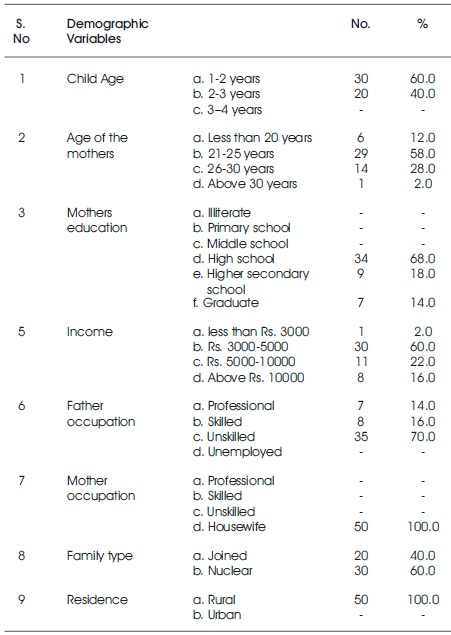
Table 1. Frequency and Percentage Distribution of Demographic Variables of the Mothers of Toddlers N=50
Behavioral problems among the toddlers are common and result from the child's need for autonomy and exploration. Toddler might like to continue to excrete whenever tension in the bowel or bladder occurs. An important part of dealing with the issue of toilet training is to educate parents about the signs of readiness for their child to begin. A pre experimental research approach and one group pre test post test design was adopted to find out the effectiveness of structured teaching programme on behavioral problems and toilet training. This study was conducted on mothers of toddlers admitted in pediatric wards at RMMCH, Chidambaram. Data were collected through structured questionnaire. The total sample comprises of 50 mothers of toddlers who full fill the inclusion criteria. This study assessed the knowledge and attitude among mothers of toddlers regarding behavioral problems and toilet training, and found that the mothers had inadequate knowledge related to behavioral problems and toilet training. The study concluded that the structured teaching programme was effective in improving knowledge and attitude of mothers regarding behavioral problems and toilet training.
Behavior problems among the toddlers are common and they only result from the child's need for autonomy and exploration. All kids are not ready for “toilet training” at the same age. So it's important to watch the child for signs of readiness. The child shows these signs between 18 and 24 months, although some may be ready earlier or later. Arrival of a new infant represents a crisis for even the best prepared toddlers. It is not the infant that toddler's hate or resent but the changes that this additional sibling produces, especially the separation from the mother during birth. Temper tantrums are nearly universal during toddlerhood as independence is established and more complex tasks are attempted that may overwhelm the child emotionally. Toddlers may assert their independence by violently objecting to discipline (Hockenberry & Wilson, 2009).
Galscoe and colleagues (Galscoe & Marks, 2011) found that parents waiting for preventive health visits rarely had concerns about their child's physical health. In total, 70% had psychosocial concerns which includes worries about: The effects of careers on children's well-being (35%); social difficulties (8% - 13%); experiencing a recent death in the family (10%); and discipline (24%). Particularly striking in the Hickson study was the fact that nearly 14% of parents had concerns about children's learning and cognition ability; a figure quite in keeping with the expected prevalence and incidence of developmental problems in childhood (Glascoe & Marks, 2011). Different cultures have different methods of toilet training and distinct expectations about when bladder and bowel control should be achieved. The strategies employed to achieve this control have changed over the last few decades: training now starts later, regular times for urination have been abandoned and the regular toilet seat without adapter and step stool to support the feet is being used instead of a potty (Schum et al., 2001; Bakker & Wyndaele, 2000). Toilet training is a developmental milestone and is a challenge to parents and children. It is one of the first steps that children take to become selfsufficient. All children will manage to acquire the necessary control eventually, but the difficulty involved is a major concern for parents and causes conflicts within the family (Schum et al., 2001).
Dworkin, Connell and Doty (2013) stated in their article about parental expectations regarding behavior along with typical management strategies surrounding conflicts and separation. Before responding to parents concern, it is crucial that the clinician be knowledgeable about ageappropriate recommendations and normal behavior and also determines what the parent's expectations are. One of the most difficult aspects of rearing children in this agegroup is persistent “no” response to every request. Negativism begins to subside as most children prepare to enter kindergarten (Glascoe & Marks, 2011). Breath-holding spells are one of the most frightening experiences parents encounter with their young children. These episodes involve the sudden cessation of breathing in response to a strong emotional stimulus. A prolonged episode may lead to unconsciousness, which are generally precipitated by a temper tantrum or other instance of frustration or anger. As the child is expressing its displeasure, there is involuntary holding of the breath during expiration. All the children are born with certain characteristics called temperament. Temperament is a set of these in-born traits that organize the child's approach to the world. These traits appear to be relatively stable from birth. Majority of babies are 'easy babies'. Generally they are quiet throughout the day. They cry only when they are hungry or discomfort but can be consoled easily. But there is always a group who are 'difficult babies' who cannot be consoled easily. These babies are prone for temper tantrums when they become toddlers and continue to become worse if they are not reared properly (Wilson & Rodgers, 2016).
The natural jealousy and resentment of children toward a new child in the family or toward other children in the family is referred as sibling rivalry (Marlow & Redding, 2000). The temperament of each child also has an influence on this training (DeVries & DeVries, 1977). Toilet training itself is complex and is accomplished in steps. Acquisition of the independence necessary to use the toilet includes: walking to the toilet or potty, sitting on it, urinating or evacuating, pulling pants down and back up, flushing, washing hands and returning to the original location. Being “ready” for this stage is important to make it more enjoyable and of shorter duration. Acquiring autonomy to use the toilet requires that the child has mastered not just language, but also motor, sensory, neurological and social skills. Climate, culture and access to disposable diapers are important factors in starting toilet training (Blum, Taubman, & Nemeth, 2003).
A study to assess the effectiveness of Structured Teaching Programme on behavioral problems and toilet training among the mothers of toddlers admitted in Rajah Muthaiah Medical College and Hospital (RMMCH) at Chidambaram.
A descriptive study was conducted by Gupta, Mongia and Garg (2017) on behavioral problems in school going children in UP. In this study five hundred children aged 6–18 years were randomly selected from a government school in Kanpur, Uttar Pradesh, and assessed for cognitive, emotional, or behavioral problems using standardized tools. Results showed that about 22.7% of children showed behavioral, cognitive, or emotional problems. Additional screening and evaluation tools pointed toward a higher prevalence of externalizing symptoms among boys than girls. The study highlights the importance of regular screening of school children for preventive as well as timely remedial measures (Gupta, Mongia, & Garg, 2017).
Ogundele (2018), reviewed relevant published literature including published meta-analyses and national guidelines. Researcher searched for articles indexed by Ovid, PubMed, PubMed Medical Central, CINAHL, EMBASE, Database of Abstracts and Reviews, and the Cochrane Database of Systematic reviews and other online sources. The research were conducted using a combination of search expressions including “childhood”, “behaviour”, “disorders” or “problems”. Behavior of children and associated emotional problems with their related disorders have significant negative impacts on the individuals, on the family members and the society as a whole. They are usually associated with poor academic, occupational, and psychosocial functioning. It is important for all healthcare professionals, especially the Paediatricians to be aware of the range of presentation, prevention and management of the common mental health problems in children and adolescents (Ogundele, 2018).
A longitudinal study on 'Age at initiation of toilet training and subsequent daytime bladder control in school-age children' was conducted in UK. The samples of the study were 8000 children, aged 4.5 to 9 years and their parents. The data was collected using a questionnaire. The researchers compared with children whose toilet training was initiated between 15 and 24 months. Result shows that In 60% of cases, initiating toilet training after 24 months is associated with problems attaining and maintaining bladder control during day time (Joinson et al., 2009).
A prospective study on 'Relationship between age at initiation of toilet training and duration of training' was conducted in Philadelphia. A total of 406 children between 17 and 19 months of age, and their parents seen at a suburban private practice were enrolled in the study which revealed that 68% of mothers are unaware of proper toilet training techniques. There was a significant correlation between toilet training and mother's level of knowledge of toilet training (Blum, Taubman, & Nemeth, 2003).
A prospective study 'To examine the incidence and age at onset of hiding while defecating in children before they have completed toilet training' was conducted in USA. Study was conducted in suburban private pediatric practice with a sample of 378 children aged 30 to 42 months. They were followed up by telephonic interviews with parents every 2-3 months, until they completed daytime toilet training. Results shown that 263 children (69.6%) met criteria for hiding groups, 38 began hiding before toilet training was initiated and 64 started hiding after intensive toilet training had begun. The non-hiders 115 (30.4%) were significant. They completed toilet training at an earlier age than hiders that is, 34.5 vs. 38.1 months (Taubman, Blum, & Nemeth, 2003).
A pre-experimental one group pretest – post test design was adopted for this study. The study was conducted in RMMCH at Chidambaram. Mothers of toddlers admitted in pediatric wards at RMMCH who fullfill the inclusion criteria are selected for the study. The sample comprise of 50 mothers of toddlers who fullfill the inclusion criteria.
5.1.1 Inclusion Criteria
Mother of toddlers who are all admitted in pediatric ward II and III and who can read and write Tamil and English. Exclusion criteria includes mothers who are not willing to participate and mothers of critically ill children.
Written permission was obtained from the Dean and the Head of Pediatric department of RMMCH. The doctor and staff nurse incharge were made aware of the nature of the study and were assured that the study would not affect their daily routine. The researcher introduced herself to the mothers and developed a good rapport with the mother.
The purpose of the study was explained to every sample, so as to get their full cooperation. The pre test knowledge was assessed by giving structured questionnaire to the mothers of toddlers for 30 minutes. 50 samples were selected using convenience sampling method to assess the knowledge and attitude regarding behavioral problems and toilet training.
The structured teaching programme was given to the same samples on the same day using flash cards for 1 hour. After 3 days post test knowledge was assessed using the structured questionnaire for 30 minutes. The collected data were analyzed.
Table 1 reveals that 60% (30) children were in the age group of 1-2 years, 40% (20) children were in the age group of 2-3 years. Regarding mothers age, 6 (12%) mothers were less than 20 years, 29 (58%) mothers were between of 21- 25 years, 14 (28%) mothers were between 26-30 years, while the remaining 1 (2%) was above30 years.
Table 1. Frequency and Percentage Distribution of Demographic Variables of the Mothers of Toddlers N=50
As far the education level of the mothers was concerned, majority of the mothers 68% (34) had education up to high school, and 18% (9) attended higher secondary school, and 14% (7) completed graduation.
While considering the family income of parents, it was found that 60% (30) subjects had income of Rs 3000-5000, 22% (11) subjects had Rs 5000-10000, 16% (8) subjects had above Rs.10000, 2% (1) subject had less than Rs.3000.
Table 2 shows that 49(98%) mothers had inadequate knowledge 1(2%) of them had moderately adequate knowledge on behavioral problems in the pre test.
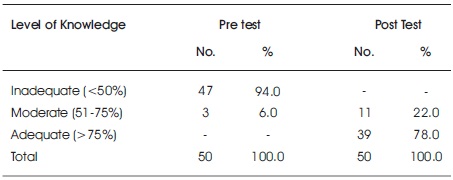
Table 2. Knowledge Level of Mothers regarding Behavioral Problems and Toilet Training in Pre test and Post test N=50
The table shows that 36 (72%) of mothers had moderately adequate knowledge and 14 (28) of them had adequate knowledge on behavioral problems in the post test.
Table 3 shows that 50 (100%) of them had inadequate knowledge on toilet training in the pre test. The Table 3 shows that 28 (56%) of them had adequate knowledge and 22 (44%) of them had moderately adequate knowledge on toilet training in the post test.
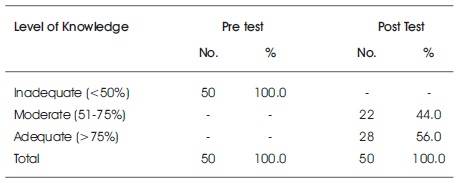
Table 3. Knowledge Level of Mothers regarding Toilet Training N=50
Table 4 reveals that on pre test all the 50 (100%) mothers were having moderately favorable attitude and none of them were having unfavorable attitude regarding behavioral problems and toilet training. This table also reveals that all the 50(100%) mothers were having favorable attitude and none of them were having unfavorable and moderately favorable attitude. It shows that there was an improvement in the level of attitude in post test when compared to pre test regarding behavioral problems and toilet training.
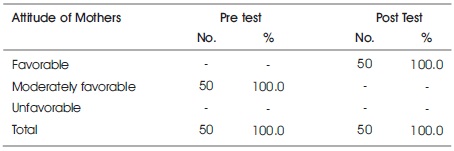
Table 4. Attitude of Mothers Regarding Behavioral Problems and Toilet Training in Pre and Post test N=50
Table 5 shows that the average pre test knowledge score among mothers of toddlers found to be 8.6200. After the structured teaching programme the mean post test knowledge score was 23.06. The standard deviation in pre and post test were 1.71298, 2.76575 respectively. Thus, the difference in level of the knowledge was confirmed by the obtained Paired 't' test value of 36.459, which was significant (P 0.000)
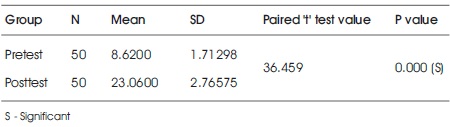
Table 5. Comparison of Mean & Standard Deviation of Pre and Post test Knowledge Score of Mothers of Toddlers regarding Behavioral Problems and Toilet Training
Table 6 shows that the mean knowledge in pretest was 1.0200 with standard deviation of 0.14142. In post test the knowledge score was 2.2400 with standard deviation of 0.47638. Thus, the difference in level of the knowledge was confirmed by the obtained paired 't' value (18.565) which was significant at p=0.000. Hence, the mothers of post test had more knowledge regarding behavioral problems after the educational programme.

Table 6. Comparison of the Mean & Standard Deviation of Pre and Post test Knowledge Score of Mothers of Toddlers regarding Behavioral Problems
Table 7 shows that the mean knowledge in pre test was 1.0000 with standard deviation of 0.00000. In post test the knowledge score was 2.5600 with standard deviation of 0.50143. Thus the difference in level of the knowledge was confirmed by the obtained paired 't' value (21.999) which was significant at p=0.000. Hence, the mothers of toddlers of post test had more knowledge about toilet training after educational programme.
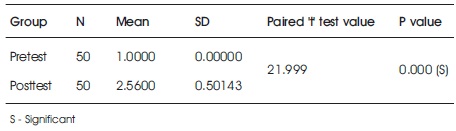
Table 7. Comparison of the Mean & Standard Deviation of Pre and Post test Knowledge Score of Mothers of Toddlers regarding Toilet Training
It is inferred from the Table 8 that the subjects having children between 1-2 years of age scored high mean value of 8.733. This difference was statistically confirmed by P value (.572) which was not significant.
The Table 8 also shows that the subjects between 21-25 years of age scored high mean value of 8.862. This difference was statistically confirmed by P value (.571) which was not significant.
On the basis of Table 8 mothers with high school education scored high mean value of 7.970. This difference was confirmed by P value (.000) which was significant.
The Table 8 shows, mothers with the family income of Rs. 3000-5000 scored high mean value of 8.000. This difference was statistically confirmed by P value (.007) which was significant.
It is evident from Table 8, that the mothers from the nuclear family scored high mean value of 8.433. This difference was statistically confirmed by P value (.351) which was not significant.
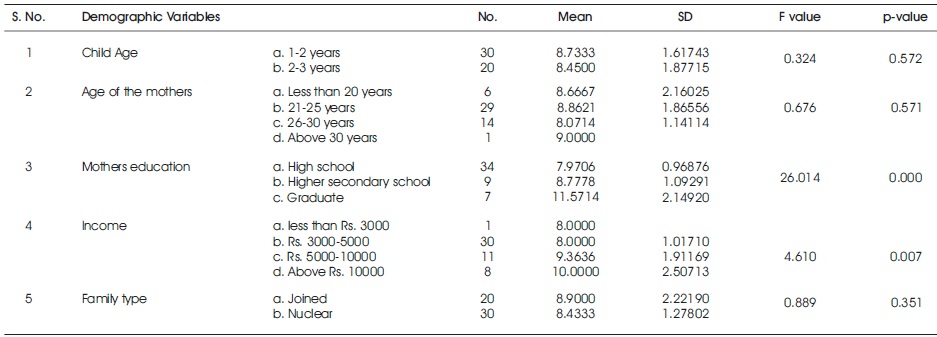
Table 8. Mean, Standard Deviation of the Mothers of Toddlers Knowledge Score with respect to their Demographic Variables
On the basis of F test result and p value (>0.000), it was concluded that the demographic variables such as mothers education and family income have significant association with knowledge of mothers of toddlers on behavioral problems and toilet training. It was also inferred that, the other demographic variables such as child's age, mother's age, education, income, occupation, and family type did not have any association with the knowledge of mothers of toddlers.
It was inferred from the Table 9 that the subjects having children between 1-2 years of age scored high mean value of 28.66. This difference was statistically confirmed by P value (.980) which was not significant.
The Table 9 also shows that the subjects between 21-25 years of age scored high mean value of 8.862. This difference was statistically confirmed by P value (.760) which was not significant.
On the basis of Table 9, mothers with high school education scored high mean value of 28.11. This difference was statistically confirmed by P value (.229) which was not significant. Table 9, shows that mothers with the family income of Rs 3000-5000 scored high mean value of 29.1667. This difference was statistically confirmed by P value (.572) which was not significant.
It is evident from the Table 9, mothers from the nuclear family scored high mean value of 28.1333. This difference was statistically confirmed by P value (.295) which was not significant.

Table 9. Mean, Standard Deviation of the Mothers of Toddlers Attitude Score with respect to their Demographic Variables N=50
On the basis of F test result and p value (>0.001) it was concluded that the demographic variables did not have any association with attitude of mothers of toddlers on behavioral problems and toilet training.
Based on the findings of the present study the following recommendations are made:
A prospective study was conducted on relationship between age at initiation of toilet training and duration of training by Blum, Taubman, and Nemeth in 2003. In this study, parents were expected to have initiated toilet training when they first took out a potty chair and discussed some aspect of training with the child. Intensive toilet training is as when asking the child to use the toilet or potty more than three times per day.
According to this study, early initiation of intensive toilet training correlates with an earlier age at completion of toilet training but also a longer duration of toilet training (Mota & Barros, 2008). Although earlier toilet training is not associated with stool withholding, or stool toileting refusal, constipation and initiation of intensive training before 27 months does not correlate with earlier completion of toilet training (DeVries & DeVries, 1977). Although toilet training is strongly influenced by cultural variations, it is universally seen as a milestone in child development, being one of the first challenges a child faces in acquiring independence. An increase in the age at which toilet training is initiated has been observed over recent decades and researchers have not accessed the true reason. Paradoxically, parents and carers report expectations of a very early age for the start of toilet training. Correct bladder and bowel voiding habits are important for a healthy life and good self-esteem. Urination and evacuation problems cause discomfort for the children and their families, and are motives for conflicts, distress and painful experiences for families and children and also during socialization at schools, when playing with friends and performing leisure activities (Joinson et al., 2009). The introduction of behavioral methods for the treatment of elimination dysfunction, such as the introduction of retraining of urination and evacuation habits, has brought good results, suggesting that well conducted toilet training may prevent future problems (Mota & Barros, 2008).
A study conducted by Lancioni, Duker, Klaase & Goossens (1994) assessed the possibility of teaching self-initiated toileting through a programme that allowed the subjects (children with severe developmental disabilities) to remain in their normal contexts and supplied these contexts with toileting cues. Frequent toileting, positive reinforcement and reprimands were also the features of the programme. The results showed that all three children participating in the study acquired self-initiated toileting. Two of them became virtually free from accidents, one continued to have a few accidents (Lancioni, Duker, Klaase, & Goossens, 1994). In the present study it was observed that mothers with high school education scored high mean value of 7.970. The P value was (0.000) which was statistically a significant difference. The mothers with the family income of Rs 3000- 5000 also scored high mean value of 8.000. This difference was also statistically confirmed by P value which was (0.007) and hence significant.
The present study assessed the knowledge and attitude among mothers of toddlers regarding behavioral problems and toilet training, and found that the mothers had inadequate knowledge related to behavioral problems and toilet training. After the structured teaching programme on behavioral problems and toilet training, there was a significant improvement on knowledge and attitude of the mothers regarding behavioral problems and toilet training. The study concluded that the structured teaching programme was effective in improving knowledge and attitude of mothers regarding behavioral problems and toilet training.