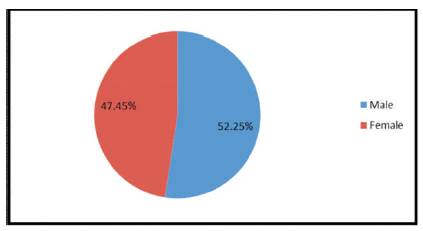
Figure 1. Excluded Children by Gender based on a surveyed sample size of 7,606 students
School attendance is essential to optimize children's education. Most minor illnesses and injuries do not warrant school exclusion, and children need to be excluded from school only for compelling medical reasons. Standardized School Health Offices (SHO) visit logs, from September to November 2010, were examined from 11 elementary and 4 middle schools in the Ocean View School District, Huntington Beach, California to determine incidence of school exclusion. Of 7,606 visits, 1,198 (15.75%) children were sent home from school due to medical reasons. The top 5 medical reasons include: (1) abdominal pain 22.62%, (2) nausea & vomiting 21.04%, (3) upper respiratory infections 14.02%, (4) headache 11.69%, and (5) injuries 7.85%. The number of exclusions in the elementary schools was significantly higher in October than in September or December. The pattern was not repeated in the middle schools. Gastrointestinal causes, conditions associated with significant pain, and contagious diseases were the top three most common reasons for exclusion from school, accounting for 89% of all exclusions. School health office personnel need to be educated on the appropriate evaluation and management of the above conditions. Over the counter pain medications should be allowed to be dispensed when indicated.
The primary mission of schools is the education of children. Students who succeed in school are more likely to become healthier and more productive adults than those students who experience academic failure[1]. Education is one of the strongest predictors of health, and the more schooling people have, the better their health is likely to be[2]. Regular attendance in school was also a significant predictor of better academic achievement [3,4]. Student exclusion due to medical reasons need to be managed better, since attendance was also a direct moderator of scholastic achievement[4]. .Therefore, it is essential that children be kept in school and not be excluded without compelling medical reasons.
Children are excluded on a daily basis from schools for multiple reasons, including medical reasons such as illness or injuries; the decision to exclude them is made by School Health Offices (SHO) personnel based on their evaluation and best judgment. Often, factors including the severity of illness or injury, the inability of a child to function appropriately and safely in school or the contagious nature of the illness are the basis on which school exclusions are determined[1]. According to the American Academy of Pediatrics (AAP), most minor illnesses do not need exclusion from school[5]. The AAP also have set standardized guidelines for school exclusions for contagious diseases. Studies on child care center reported, high percentage of unnecessary exclusion placed a significant high burden on families, business, and health care resources [6-8]., however, there is a limited number of studies on school exclusions due to medical reasons in elementary and middle school children in the US. In this study, we assess and quantify the medical reasons for school exclusions in elementary and middle schools and determine the top five medical reasons and seasonal pattern of these exclusions.
A retrospective chart review was conducted to 7,606 visits to explore the incidence and categories of health care problems in kindergarten through eighth grade students while they were in school. The study analyzes school nurse visit logs of children attending the Ocean View School District (OVSD) in Huntington Beach, California. All the schools had a School Health Office, staffed by either a school nurse (Registered Nurse) or a Health Technician. The variables being studied are the number of official visits by the school children, time of the visit, the medical reasons for the visit, and whether or not these children were excluded (sent home) based upon the nursing diagnosis.
There were 9,159 children enrolled in the OVSD during the 2010-2011 academic year. This school district has 11 elementary schools from Kindergarten through 5th grade and 4 middle schools from 6th through 8th grade. The health logs were collected between September 9th, 2010 and November 30th, 2010. There were 53 school days during this period with an average daily attendance of 8,965 students. Of the 9,159 children, there were 7,606 visits to the school nurse due to illness or injury during the surveyed period. 15.75% or 1,198 children of those 7606 visits were sent home.
Prior to starting data review, permission was obtained from the School Board of the Ocean View School District and was deemed exempt from the District Institutional Review Board. Data were obtained from the standardized health logs completed by the SHO personnel. The inter-rater reliability score of 95% was obtained by having the school nurses and the PI score 10 randomly selected records and calculating agreement between the two scores.
The logs—detailed under instruments— were designed to capture the gender, age, ethnic group, grade, medical reasons for presentation to the SHO and the disposition of the child following evaluation. To ensure security and privacy of the participants, no personal identifiers were collected. Only children who were excluded from school due to illness or injury were included in the analysis. Children who presented for non-medical reasons such as emotional or behavioral problems, social issues, and normal physiological processes such as thirst, hunger and normal menstrual periods were excluded. Children who presented for routine screening for vision, hearing or scoliosis and for the administration of prescribed medications, but were otherwise healthy were excluded. If a child presented with multiple symptoms, the chief complaint was used in the classification. If a child presented multiple times in a single day for the same complaint, only the initial visit was included in the analysis.
Following an initial review of the health office visit logs, the school exclusions were classified into 15 categories which were injuries, abdominal pain, headache, nausea and vomiting, upper respiratory infections, asthma/bronchitis, insect bites, non-traumatic pain, conjunctivitis, earache, toothache, skin rash, epistaxis, lice infestation and miscellaneous reasons. The miscellaneous category captured data which included non-specific fevers, dizziness and child looking or acting sick. Children who were excluded due to cough, rhinorrhea and sore throat were classified as upper respiratory infections, pink eyes due to allergies or infections were classified as conjunctivitis. Non traumatic pain included pain in the extremities, neck, chest, and back not due to trauma. Only the principal investigator (a Board Certified Community Pediatrician) reviewed and classified the school exclusions in the logs into disease categories. After re-categorization of the clinical presentation, data documenting exclusions and inclusions for school attendance was collected and evaluated.
The instrument consisted of a questionnaire that had two parts: Part I included demographic data, including: age, gender, ethnicity, grade level, and exclusion status. Part II included a list of the following 15 categories of physical ailments: 1) Injuries, 2) Abdominal pain, 3) Headache, 4) Nausea and vomiting, 5) Upper respiratory infection, 6) Asthma/bronchitis, 7) Insect bites, 8) Non-traumatic pain, 9) Conjunctivitis, 10) Earache 11) Toothache, 12) Skin rashes, 13) Epistaxis 14) Lice infestation, and 15) Miscellaneous causes that captured data which included non-specific fevers, dizziness and child looking or acting sick.
The descriptive analysis was performed for the first part of the log (demographic data, time of visits, and exclusion status) and the incidence was calculated by counting the number of cases in each category obtained from the second part of the log. Children who presented with symptoms such as cough, rhinorrhea and sore throat were classified as upper respiratory infections. Pink eyes due to allergies or infections were classified as conjunctivitis. Viral exanthemas, impetigo, eczema, allergic rashes and head lice were classified as skin rashes. Non traumatic pain included pain in the extremities, neck, chest, and back not due to trauma. The data were entered, tabulated, and analyzed using SPSS 19 statistical package software.
The survey was conducted from September 9th 2010 through November 30th 2010. There were 53 school days during this period. During the academic year 2010-2011, there were 9,159 children enrolled in the 11 elementary schools and 4 middle schools in the OVSD. The average daily attendance was 8,965. During the survey period, 7,606 children visited the SHO due to illness or injury of whom 1198 (15.75%) children were sent home (excluded). 52.25% of them were male and the majority of them (43.84%) were 13 years old (See Figure 1 and 3). More than half (54.26%) were Caucasian, 30.3% were Hispanics, 10.6% were Asians, .83% were African Americans, and 4.01% were Others (declined to state ethnicities) (See Figure 2).
Figure 1. Excluded Children by Gender based on a surveyed sample size of 7,606 students
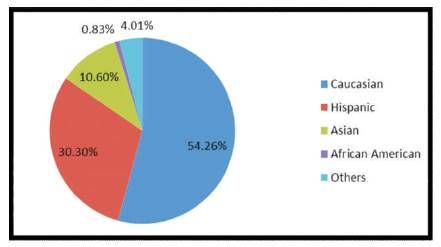
Figure 2. Excluded Children by Ethnicities based on a surveyed sample size of 7,606 students
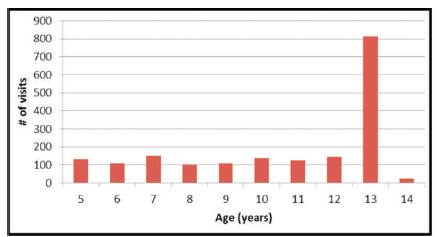
Figure 3. Excluded Children by Age based on a surveyed sample size of 7,606 students
Of the 1,198 children who were sent home (excluded), the top five medical reasons for the exclusion from school were abdominal pain (22.62%), nausea and vomiting (21.04%), upper respiratory infections (14.02%), headache (11.69%), and injuries (7.85%). Details of the rank order of each category are shown in Table 1.
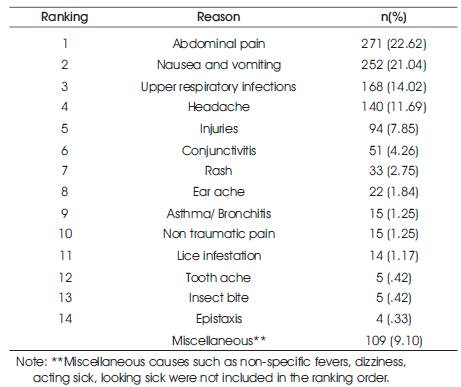
Table 1. Medical reasons for exclusion in rank-ordered (n = 1198)
Of the 7,606 visits to the SHO, the top five medical reasons to visit the SHO were injuries (35.46%), abdominal pain (16.47%), upper respiratory infections (8.57%), headache (7.51%), and nausea and vomiting (5.59%). However, of the 2,697 visits (35.46%) that were caused by injuries, there were only 94 children (3.49%) who were sent home. On the other hand, of the 425 visits (5.59%) that were caused by nausea and vomiting, 252 (59.2%) children were sent home.
Ranking of percentage of exclusion of total presentation to SHO by each category is shown in Table 2 below.
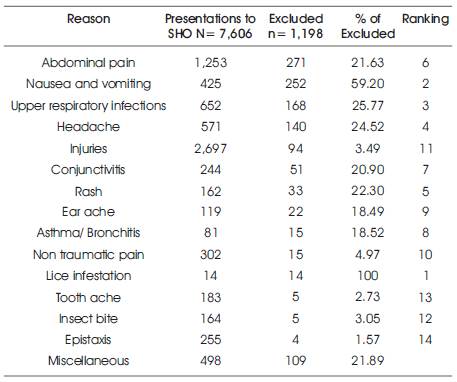
Table 2. Percentage of exclusion of total presentation to SHO by each category
Of the 750 total exclusions in elementary schools, there were 305 visits (40.67%) that occured in the month of October, 32.8% in September, and 26.5% in November. On the other hand, of the 443 total exclusions in middle schools, they were almost equally spread over those three months, 29.7% in September, 33.77% in October, and 35.66% in November (See Table 3).
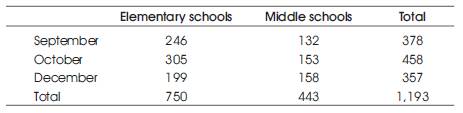
Table 3. Number of exclusion by school level and time of presentation (month
Abdominal pain was the most frequent single symptom for school exclusions (22.62% of total exclusion) in elementary and middle school children and the second rank of the medical reasons visiting the SHO (16.5% of total visits to SHO were caused by abdominal pain). According to a study by Youssef et al, recurrent abdominal pain affects up to 15% of school aged children who face significant psychosocial consequences including school absences[9]. .The majority of recurrent abdominal pain in childhood was caused by functional/non-pathological etiology [10, 11]. Studies indicated that school nurses were not clear on epidemiologic and etiologic features of recurrent abdominal pain and had negative views that may inadvertently contribute to the anxiety felt by affected children [9]. Therefore, further studies to ascertain the reasons for the high incidence of abdominal pain in this population and strategies to handle functional abdominal pain need to be developed. Education of school nurses and communication from physicians may advance strategies designed to reduce the fiscal and social costs associated with this common childhood condition[9].
Contagious illnesses that include Upper Respiratory Infections (URI) 14.02%, conjunctivitis 4.26%, rash 2.75%, and lice infestation 1.17% accounted for a total 22.02%. It was the second single cause of exclusions after abdominal pain and nausea and vomiting. The URI itself were the third rank of causes to visit the SHO. To reduce the incidence, education of children regarding hand washing and personal hygiene is indicated which is essential to prevent the spread of communicable diseases to others[12].
Nausea/vomiting was the third leading cause for school exclusions (21.04%). However, it was the second rank of percentage of exclusion presenting to the SHO. 59.25% children who visited the SHO with nausea and vomiting were sent home (excluded). It is apparent that SHO personnel were not comfortable with managing nausea/vomiting in the SHO. An education program for SHO personnel regarding evaluation and management of Nausea/vomiting in childhood may result in the decrease of school exclusions due to this cause.
Though injuries were the number one reason for presentation to the SHO (n=2697, 35.46% of all presentations), the majority of injuries were minor and only a small number of children (3.49%) were excluded from school. This finding is counter to findings in other studies that showed that school injuries accounted for 10-25% of the presentations to the SHO[13]. One of the possible explanations for this discrepancy is that injuries might not all be reported or they might be reported as other symptoms. A study looking at injuries in Elementary school children found that most injuries were misrepresented in reports because they were categorized as symptomatic pain such as headache [13] .
All other symptoms of pain other than abdominal pain were combined and accounted for 23.05% of children excluded from school in our study. These symptoms included: headaches 11.69%, Injuries 7.85%, ear aches 1.84%, toothache 0.42%, and extremity pain 1.25%. This is a significant finding because of the impact of pain on children’s well-being. In fact, the AAP policy statement acknowledges that pain in children is inadequately treated and that health care providers need to treat pain effectively [14] . However, according to the AAP and NASN, SHO personnel cannot dispense OTC pain medications to children without written consent from both the parent and the child's doctor [1][15]. The withholding of pain medications for a child in significant pain is a departure from the standard of care in outpatient health offices. The administration of OTC pain medications may or may not decrease the incidence of school exclusions, but it will certainly mitigate the pain. The current California law is a significant barrier for the administration of OTC pain medications to children in California and this barrier needs to be re-examined in order to allow for a better health management of children in Elementary and middle schools.
It would be of great significance to further our arguments to collect data on schools medical exclusions and academic achievements. We propose that schools with less medical exclusions have greater academic achievements than schools with greater medical exclusions. This future study would take the point of view based on the existing literature on health and academic performance that healthier students make more scholastic students. The conceptual framework would also take into consideration and collect other variables such as income. But once these variables are isolated, we propose that a reduction of exclusions and a more involved in-school health office managed by an APRN would decrease the number of unnecessary exclusions which would in turn increase student academic achievements.
This research contributes to the body of knowledge in nursing and promotes evidence based practice which is a core value of the American Academy of Nurses. Importantly, this research makes a case for having Advanced Practices, as Nurses become part of the collaborative effort to assess and manage the clinical care of our elementary and middle school populations. Documenting the need for Advanced Practice Nurses within our public school systems through publication will increase the awareness of legislators and nursing administrators. With greater awareness of school exclusions and new approaches to reduce them, we can improve health services and indirectly enhance the learning potential of our elementary and middle school student body.
We suggest having advanced practice nurses within the school system. With this policy change, many of the students who are sent home could be evaluated and managed with appropriate measures and be able to stay in school which is essential to their academic future. In addition, a comparison with other school health policies for exclusions across the nation and beyond our borders would be interesting to define the different processes and identify a model of best practice. One would have to be careful in making policy inferences using comparisons from different systems as this can be biased with many confounding factors, however this research method is very much encouraged by governments and health policy makers[16]
The contribution to school nursing practice is important as it shows that the clinical reasons for children's exclusion from school within the California School District need a policy revision in order to enhance health and to promote the direct outcomes of improved health. The better we document what is happening in each school and community, the better we can prepare school nurses to deliver appropriate quality health care to our school age children.