 - Arnold Bennet
- Arnold BennetTo assess the knowledge of postnatal mothers regarding postnatal depression and to find the relationship between the knowledge regarding postnatal depression with selected demographic variables such as age of mother, number of children, educational status of mother, educational status of husband, occupation of mother, occupation of husband, religion, type of family, family income per month and previous history of postnatal depression. To develop an information booklet regarding the prevention of postnatal depression. A descriptive Study was conducted among postnatal mothers regarding postnatal depression in hospitals of Moga (Punjab). A non probability convenient sampling technique was used to select 200 postnatal mothers of 19-35 years of age group. Demographic variables of study were such as age of mother, number of children, educational status of mother, educational status of the husband, occupation of mother, occupation of husband, religion, type of family, family income per month and previous history of postnatal depression. A self structured questionnaire containing 30 items was utilized to assess the knowledge regarding postnatal depression. The conceptual frame work of study was based upon Orem's Self Care Theory (1959). An educational booklet on postnatal depression among postnatal mothers was developed after analysis. The data were analyzed by descriptive (mean, median & mode) and inferential (ANOVA & correlation) statistics. Results of the study revealed that 28.5% of postnatal mothers were metric passed, 37.5% of their husbands were higher secondary passed, 76.5% of postnatal mothers were house maker, and 51.5% of their husbands were in their own business, 50% of postnatal mothers were Hindu and 50% were Sikh. Whereas 52.5% postnatal mothers live in a joint family, 69% of them had family incomes ≤ Rs.5000 and 100% of postnatal mothers had no previous history of postnatal depression. 53% of the postnatal mothers were in the age group of 23-26 years, 47% of postnatal mothers were having one child followed by 66% of postnatal mothers had below average knowledge and 32.5% of them had average knowledge. Only 1.5% of postnatal mothers had good knowledge regarding postnatal depression. In the present study, age of mother, number of children, educational status of mother, educational status of husband, occupation of mother, occupation of husband, religion, family income per month had significant impact on the knowledge of postnatal mothers regarding postnatal depression but type of family had no impact on the knowledge of postnatal mothers regarding postnatal depression.
“The best cure for worry, depression, melancholy, brooding, is to go deliberately forth and try to lift with one's sympathy the gloom of somebody else"
- Arnold Bennet
Pregnancy is one of the most exciting and important events in each woman's life. Pregnancy is a developmental challenge and a turning point in a family's life. It is the transition period from childhood to parenthood. Parenthood brings significant changes for a couple. Routines and family dynamics are altered by pregnancy. Pregnancy, birth and early parenthood are times of great change. Having a baby can be the biggest life change that any mother will ever have. In fact, for many women, having a baby is the most significant life-changing event they will ever experience [1]. Adjusting to this major life change, as well as coping with the day-to-day stress of a new baby, can make some women more likely to experience depression at this time, particularly if they have experienced depression in the past. Feelings of anxiety, irritation, tearfulness, and restlessness are common in a week or two after pregnancy. These feelings are often called the postpartum or baby blues [2] . These symptoms almost always go away soon, without the need for treatment [3]. Depression in the postnatal period has a major influence on the health of both mother and child. Its also has an impact on the growth and development of the child. The World Health Report 2001 identified depressive disorders amongst women in the 15 to 44 year age group as the second leading cause of disability adjusted life years (DALY) [2]. Postnatal depression is at least twice as widespread as thought, new research reveals. One in five women suffers from postnatal depression [4] . More than 4,000 women discovered one in five had suffered postnatal depression - double official statistics - while at least two thirds had felt some form of postnatal blues, and many had suffered in silence. Postnatal depression is a severe condition that has been described as "a thief who steals maternity"; up to 50 percent of the cases are diagnosed, and approximately 49 percent of women who seek help feel desperately depressed [5] . Postnatal depression is a major health issue affecting up to 13 percent of all new mothers throughout the world, with most cases beginning in the first three months of the postnatal period [6] . According to two studies prospective pregnant women in the states of Goa and rural south India, detected depressive disorder in 23 percent and 16 percent respectively, with depression persisting six months after child birth in 11-15 percent women [7] . According to screened community based postpartum depression in the first month of delivery at Massachusetts, United States of America, the findings show that the prevalence of postpartum depression to be about 19.7 percent. They have recommended detection of postpartum depression by adapting research based screening approaches to clinical care [8] . Depression in postpartum period has been classified into three categories in ascending level of severity, that is, postnatal blues, postnatal depression and postnatal psychosis. Because the blues are self limiting and the florid postpartum psychosis obvious, the serious but more often under recognized middle category becomes an important subject of enquiry [9] . Postnatal blues are a temporary and specific affective syndrome associated with childbirth. It affects between 25% and 80% of women, and is characterized by mild dysphoria, tearfulness, irritability, anxiety and mood lability. It tends to peak between the third and fifth postnatal days and is related primarily to hormonal fluctuations associated with childbirth. The prevalence of the postnatal blues, which are mild, transient and very common disturbances of postnatal mood, does not appear in a major way to be related to environmental, social or cultural factors [10] . Mood and anxiety disorders are common in women during their childbearing years.
Pregnancy and postnatal period are considered to be relatively high-risk times for women with pre-existing psychiatric illnesses, especially for depressive episodes in women. The prevalence of depression has been reported to be between 10 and 16 percent during the pregnancy. Pregnancy and postnatal period appears to confer an even greater risk for women with bipolar disorder. Risk of relapse is estimated at 30-50 percent during the postnatal period [12] . A study stated that postnatal depression is a serious mental health problem for women and its consequences have important implications for the welfare of the family and the development of the child. Symptoms include sadness, fatigue, insomnia, appetite changes, reduced libido, crying episodes, anxiety, and irritability [13]. Profound hormonal changes after childbirth are often claimed to cause postnatal depression, and there is little evidence that variation in pregnancy hormone levels is correlated with variation in postnatal depression levels [14]. Mental health is “the adjustment of human beings to the world and to each other with a maximum of effectiveness and happiness”.
Postnatal depression is a form of clinical depression which can affect women, and less frequently men, after childbirth. Kit LK et al. reported prevalence rates among Indian women from 5 percent to 25 percent. Postnatal depression was 3.9 percent. Indians had the highest rate at 8.5 percent as compared to Malays (3.0 percent) and none in Chinese (p < 0.05). There were no demographic differences in the study groups. Average score of the Edinburgh postnatal depression scale was 4.05 which ranged from 0 to 20. During the confinement 85.7percent of women took special diet; 64.3 percent and 78.8percent had someone to look after them. The incidence of postnatal depression is low in Malaysia at 3.9percent [15] . Indian women are major victims of postnatal depression as they are not aware enough to develop coping up strategy. An awareness programe is of prime importance for Indian women. A total number of 500 women were studied in a survey and was found that 33 % of Indian women had no knowledge about postnatal depression and 12% never heard about it. There was significant difference between the postnatal mothers of 16-33 years and >34 years [16] .
Conceptual Framework is made of concepts, which are words describing mental images of phenomenon & predisposition which are stating about the concepts. A conceptual model of framework therefore is defined as, a set of concepts & predisposition that integrate them into a meaningful configuration. The framework of the present 17 study is based on Orem's Self Care theory (1959). Orem presents four conceptual concepts.
It is the behavior that exists in concrete life situations directed by persons to self or to the environment to regulate factors that affect their own development and functioning in the interest of life, health or well being.
It is the human's ability or power to engage in self-care. In this study, self-care agencies are the samples of the study i.e. postnatal mothers with live babies, hospitalized or visited the hospital within 45 days after the delivery, who can take care of themselves, but the postnatal mothers ability to engage in self care can be affected by the conditioning factors such as age of mother, number of children, educational status of mother, educational status of husband, occupation of mother, occupation of husband, religion, type of family, family income per month and previous history of postnatal depression.
It delineates when nursing is needed. Nursing may be provided if the core abilities are less than those required for meeting a known self care demand or predictable decrease in the core abilities. In this study inadequate knowledge of postnatal mothers regarding postnatal depression is the self-care deficit.
It is the totality of self care actions to be performed for some duration in order to meet self care requisites by using valid methods and related sets of operations and actions. In this study, self care demands refer to maintaining proper hygiene, establishing interaction with neonate, proper care and support of spouse and family members, recreational activities, nutritional diet, regular exercise, calm and quite environment.
Describes and explains the relationship that must be brought about and maintained for nursing to be performed. Three nursing systems are described by Orem based on the dependency; they are wholly compensatory, partly compensatory and supportive-educative system. In this study, postnatal mothers have the ability to meet their self-care need with proper guidance, support and teaching. They can be beneficial for themselves and also for others. Thus, in this study, postnatal mother belongs to the supportive educative system as per nursing system. So education and guidance was imparted through developing information booklet (Figure 1).
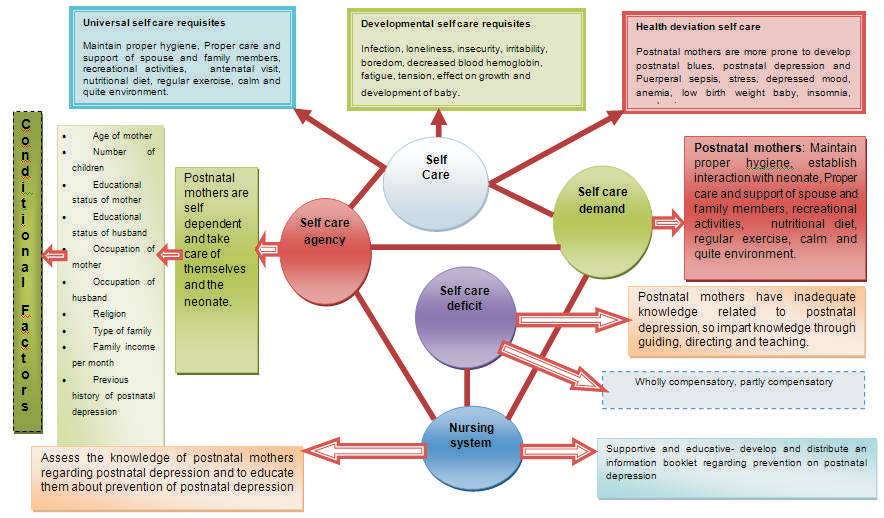
Figure 1. Modified Conceptual framework based on Orem's Self Care Theory (1959)
A quantitative/non experimental research approach was adopted to accomplish the objective of the study.
In the present study, Descriptive research design was utilized to assess the knowledge among the postnatal mothers regarding postnatal depression, according to selected variables like age of mother, number of children, educational status of mother, educational status of the husband, occupation of mother, occupation of husband, religion, type of family, family income per month and previous history of postnatal depression.
The present study was conducted in Civil Hospital and Mittal Hospital of Moga. Civil Hospital Moga has facilities with 150 beds and separate gynae wing in the campus including both indoor and outdoor facilities for patients. The Mittal hospital has a facility of 100 beds with the specialty of Obstetrics and gynae. Criteria for selecting these settings were that the investigator was familiar with the hospital. Administrative approval was taken before carrying out the final study.
The investigator is selected sample size was 200 postnatal mothers. These mothers were selected by convenient sampling technique. The criteria for selection were postnatal mothers with live babies, in the age group of 19- 35 years & hospitalized or visited the OPD of civil hospitals or Mittal hospital of Moga (Punjab).
Tool consists of the following parts:-
The part consists of items of obtaining personal information about subjects such as age of mother, number of children, educational status of mother, educational status of the husband, occupation of mother, occupation of husband, religion, type of family, family income per month and previous history of postnatal depression.
This part consists of multiple choice questions regarding postnatal depression. A total of 30 questions is included and each right question carries one mark & each wrong question carry 0 marks.
Content validity refers to the adequacy of the domain being studied. Content validity of the tool was confirmed by the expert's opinion regarding the relevance of the items. The structured tool regarding postnatal depression was circulated among experts from various fields of specialization such as 9 from psychiatric nursing service, 1 from Maternal and Child Health Nursing, and 1 from psychiatrists. Their valuable suggestion was obtained and incorporated. The final tool consists of 2 parts after the necessary changes done. The knowledge score was finalized with 30 items. Reliability refers to the accuracy of the measuring tool. Reliability of the tool was estimated by Split half technique which included computing Pearson's coefficient of correlation and thereafter by applying Spearman Brown Prophecy formula, which was found to be r = 0.8 for Structured questionnaire. Hence the tool was highly reliable.
Data collection was done in the month of February 2011. The sample consisted of 200 subjects. The Convenient sampling technique was used to select a sample from the population. Prior to data collection, formal permission was obtained from Senior Medical officer of Civil Hospital of Moga and Doctor incharge of the Mittal hospital of Moga, Punjab. Prior to handling over the questionnaire to postnatal mothers, investigator gave a self-introduction to the postnatal mothers and explained the purpose of gathering information. They were assured that their responses will be kept confidential and used only for research purpose & consent was taken from postnatal mothers. The time taken by each respondent for filling the questionnaire was an average of 20-25 minutes.
Analysis and interpretation of data were done by using descriptive and inferential statistics such as Percentage, Mean, Mean Percentage, Standard Deviation, Coefficient of Correlation, and Anova. Pie and bar diagrams were used to depict the findings of the study.
In the present study, highest numbers of postnatal mothers (53%) were in the age group of 23-26 years followed by the majority of postnatal mothers(47%) having one child. In the present study, highest numbers of postnatal mothers (28.5%) and their husbands education (37.5%) was metric & higher secondary. In this study, majority of postnatal mothers (76.5) were house makers followed by large numbers of husbands (51.5%) who were businessmen. The religion of postnatal mothers in the present study was equally distributed (50, 50%) in Hindu and Sikh religion followed by 52.5% postnatal mothers belonging to joint family. Large numbers of postnatal mothers had ≤ Rs. 5000 monthly income & no other mother had previous history of postnatal depression (Table 1).
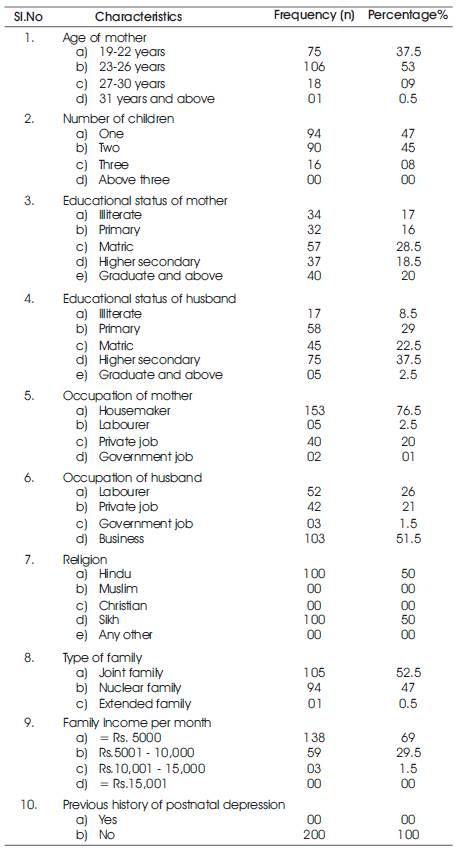
Table 1. Sample characteristics
The 1st objective was concerned with assessing the knowledge of postnatal mothers regarding postnatal depression. The findings of the present study indicated that 66% of postnatal mothers had below average knowledge, 32.5% had average knowledge and only 1.5% of them had good knowledge.
The 2nd objective is to find the relationship between the knowledge regarding postnatal depression with the selected demographic variables such as age of mother & number of children that had a significant relation with knowledge of postnatal mothers regarding postnatal depression at p<0.05, 0.001 levels. Educational status of the mother & educational status of husband had a significant relation with knowledge of postnatal mothers regarding postnatal depression at p< 0.001 level, followed by occupation of mother, occupation of husband also had a significant relation with knowledge of postnatal mothers regarding postnatal depression at p<0.001 level. Religion of mothers and the family income had a significant relation with knowledge of postnatal depression among postnatal mothers at p<0.01 & 0.001 levels. Type of family & previous history of postnatal depression had no significant relation with knowledge of postnatal mothers regarding postnatal depression.
The 3rd objective was to develop an information booklet regarding the prevention of postnatal depression. A booklet on postnatal depression among postnatal mother was compiled. Content was compiled by giving primary insistence upon deficit areas of knowledge regarding postnatal depression highlighted in the analysis of the study. Booklets were distributed among all postnatal mothers included in the study as well as other postnatal mothers attending OPD & who were hospitalized up to two days after the study.
This study deals with the assessment of knowledge among postnatal mothers regarding postnatal depression in selected Maternity hospitals of Moga, Punjab. The present study was conducted in Civil Hospital and Mittal Hospital of Moga. Total samples were 200 postnatal mothers. The Convenient sampling technique was used to collect the sample. Before collecting, data investigator gave brief introduction about self, purpose of the study and instruction regarding filling of questionnaires and gained confidence. A written consent was taken before collecting the data. The data revealed that out of 200 samples, 66% of postnatal mothers had below average knowledge, 32.5% had average knowledge and only 1.5% of them had good knowledge. In the present study, age of mother, number of children, educational status of the mother, educational status of husband, occupation of mother, occupation of husband, religion, family income per month had significant impact on the knowledge regarding postnatal depression among postnatal mothers, but type of family & previous history of postnatal depression had no significant relationship with knowledge of postnatal depression among postnatal mothers (Table 2).
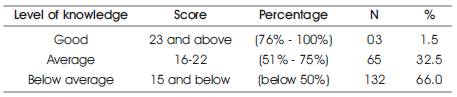
Table 2. Frequency & percentage distribution of knowledge scores of postnatal mothers regarding postnatal depression
Ethical Considerations: With the view of ethical consideration, the researcher obtained written permission from Senior Medical officer of Civil Hospital of Moga and Doctor incharge of the Mittal hospital in Moga, Punjab. Also, the postnatal mothers were explained about the purposes of the study and consent was taken from them for their participation.
With profound gratitude, the authors express their heartfelt veneration towards invaluable family and friends for enlightening guidance, interest, valuable suggestions and consistent encouragement at all stages of work. The authors deeply appreciate the untiring and outstanding contribution, encouraging words and everyday help provided by them. They also express their sincere gratitude to their mentors and teachers who guided all the way for compiling this research paper.