Table 1. Instructors Guide for Phase One
Adequate preparation of preceptors is essential to achieving optimal student learning outcomes. While several noteworthy programs are described in the literature, few if any afforded participants ongoing support. This article describes an alliance formed between faculty in a baccalaureate program and clinical nurse educators of an acute care facility. The purpose of the partnership was to facilitate preceptor success using funds received from an internal grant. The preceptor development program was an innovative approach that consisted of three phases: face-to-face, online supplemental education, and on-site clinical support. Each phase was developed based on an applicable theory of learning. Positive feedback was received from participants and faculty. Research on the effectiveness of this three-tiered approach is recommended.
High-quality effective learning experiences during preceptorship rotations are dependent upon nursing students being paired with preceptors who are proficient in managing patients with complex conditions. The Institute of Medicine's (IOM) Report on the Future of Nursing identified that quality and patient safety is impacted by the education and training of nurses. As a result of these findings, the IOM has recommended an increase in nurses with a baccalaureate degree (Institute of Medicine, 2010). According to the American Association of Colleges of Nursing (AACN), (n.d) “learning to perform as a 'nurse' is predicated on engaging in experiential learning” (p.31). Consequently, nurse preceptors must also be able to facilitate nursing students' ability to adequately connect theory to practice.
A preceptorship is a model of clinical teaching in which a nursing student is paired with a registered nurse who is responsible for the direct supervision of the student's performance (Billings & Halstead, 2012; Shepard, 2010). The barrier identified by faculty in one pre-licensure baccalaureate nursing program was many of the assigned preceptors had not been adequately prepared to assume the role. During routine site visits, faculty found that several nurse preceptors were not familiar with the principles of teaching and adult learning, while others had difficulty translating the principles into relevant and meaningful teaching strategies. A few preceptors did report attendance in a preceptor class but the focus was on how to precept new graduate nurses. As a result, some had difficulty in distinguishing which tasks were appropriate for delegating to a student nurse versus a new graduate licensed nurse.
Positive experiences in the clinical setting are critical to learning and the literature is well documented in the benefits of well established preceptorship programs (Shepard, 2010; Udlis, 2008). A research study on student's perceptions of the effectiveness of preceptorship found that, precepting is a central component of the enhancement of core competencies such as verbal and written communication skills, self-confidence, professionalism, and nursing skills (Shepard, 2010). Recognition of such significant impact raised the concern over the preceptor deficiencies identified. Dialogue between faculty, clinical leaders, and clinical nurse educators confirmed suspicion that no formal program, course, or self-directed learning activities were available for training nurses to function as preceptors for nursing students.
The disclosure of the gap in formal preceptor training opportunities initiated further conversation between faculty and clinical nurse educators on how to reconcile the problem. Literature reviews were conducted and the preponderance of the findings were single modes of training strategies offered in the form of either online selfdirected modules or one day face-to-face class session (Schaubhut & Gentry, 2010; Zahner, Tipple, Rather, and Schendzielos, 2009) . In addition, it was noted that the end of the course marked the end of support to the preceptors. Continued discussions led to a joint application between faculty and clinical nurse educators for grant funding through the hospital's internal professional grant program.
Unlike traditional single-mode of delivery programs, as identified in the literature, the grant proposal aimed to take a novel approach for developing a preceptor program. The design was blended with three phases; face-to-face class, online follow-through, and on-site real time support. All three were developed and carried out collaboratively.
The criteria for enrollment was endorsed by the participant's nurse manager, holding at least a Bachelors in nursing (BSN), having at least one year experience, and agreeing to enroll with the hospital to function as a preceptor for a baccalaureate nursing student for a minimum of 120- hours. The grant was approved without stipulation. As an added bonus, the course was eligible to offer the participants, Continuing Education (CE) hours. A Continuing Education Specialist was assigned to work with the educators and ultimately approved 3.25 CE hours for completion of the first phase which was the didactic portion of the program. The course was advertised primarily by word of mouth and flyers. Other methods included email announcements using the hospital's group email distribution lists and verbal announcements made at clinical leaders meetings.
The program was designed to take place twice during an academic year in early fall and early spring. The choice of timing was two-fold; 1) to coincide with start times of student clinical rotations so that participants would have the opportunity to immediately apply new knowledge in practice and 2) each phase would be built on the previous one, thus providing a natural progression.
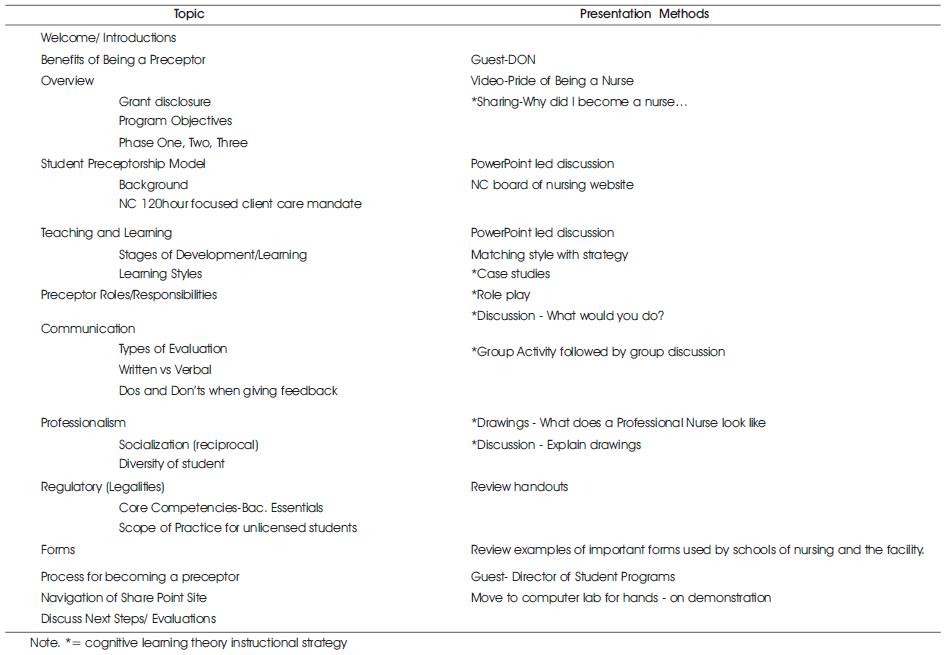
Phase one was developed based on the premise of cognitive learning theories, specifically, constructivism that suggests learning is the result of building on current knowledge ( Billings & Halstead, 2012, Chapter 13).This was believed to be most appropriate because all participants were registered nurses with baccalaureate degrees and were once students themselves bringing prior knowledge and experiences associated with clinical instruction. Instructional approaches most applicable with cognitive learning theories involve strategies that promote meaningful discussions. Examples are case studies, group interactions, role play, journaling, and drawings used to promote reflection. As shown in Table 1, titled Instructors Guide for Phase One, course content was taught using teaching strategies consistent with cognitive learning theories.
The Director of Student Programs and the Director of Nursing Practice Education and Research, both prominent figures of the hospital, were invited to speak at each session to offer inspirational support, discuss process for being assigned students, expectations, and general policies.
Phase two was the online portion of the program; it began immediately after phase one and remained available through the end of the academic year. The purpose for the online follow through was to provide additional resources, peer support, keep them engaged in dialogue, and continued self-directed learning. The learning theory that guided this development was Malcolm Knowles' androgogy that assumes adults to be self-directed and takes accountability for learning information that will be readily used ( Billings & Halstead, 2012, Chapter 13).
A share point site through the hospital was created and used as the platform. The site was redesigned to mimic an online classroom. Components of the site included links to various resource websites such as the board of nursing, the University's nursing student handbook, and the American Association of Colleges of Nursing (AACN) Baccalaureate Essentials.
Table 1. Instructors Guide for Phase One
In an attempt to keep participants engaged, a discussion board was created. Two relevant questions were posed with clear and concise instructions on posting requirements. An additional discussion thread was created for participants to ask questions of each other and instructors or to simply share experiences. Because the CE hours were limited to the first phase of the program, there could be no requirements for participation in phase two although highly encouraged. So, as a means to attract participants to the site, a photo gallery was created and populated with pictures taken during the face-to-face session.
Phase three was perhaps the most appreciated by participants. This phase ran concurrently with phase two and began immediately after a nursing student was assigned to them for a preceptorship rotation. Participants were instructed to upload to the share point site, a calendar indicating the unit, date, and times the preceptee would work. The faculty and clinical educators selected pairs to mentor for the duration of the preceptorship rotation. Then based on the schedules, planned periodic site visits were made for the purpose of offering support to the preceptor. The number of visits vary depending on the perceived need. The type of mentoring activities offered during each site visit was being available for questions, offering advice, and problem solving. The preceptor was given praise and positive reinforcement at every opportunity during the site visits in an effort to boost confidence in performance. Needless-to-say, behavioral learning theory guided the development of this phase. The premise of behavioral theories is that behavior is shaped by positive reinforcement and reward ( Billings & Halstead, 2012, Chapter 13).
During the course of planning and implementing this novel approach to a preceptor development program, it was evident that nurses who were considered to be an expert in the practice setting were usually not expert in applying principles of teaching and learning. Preceptor programs are found to be effective means for helping nursing students transition to practice; however, the ongoing success of these programs are dependent on providing support and training for preceptors (Zahner, Tipple, Rather & Schendzielos, 2009) . An evaluation of the overall planning and subsequent implementation of the described program surfaced a few barriers to success, some avoidable and others not within the control of the facilitators.
Issues out of the facilitators' control were the high number of new graduates in hospital orientation at the time the program was offered and the number of hospital-wide mandated educational projects taking place concurrently. A few nurse managers verbalized support for the program and shared that they received numerous requested from nurses to be enrolled, however, due to the strain of resources, they were forced to decline the requests for the first session.
The targeted groups of staff nurses work on set six-week tracks that are planned at least two weeks before the first day on the schedule. Since nurse managers encourage staff nurses to plan class attendance time around work schedules without disrupting the unit coverage, it is critical that dates for classes are planned and published at minimum two months in advance. Advertisement of dates for this program was disseminated two weeks before the first offering creating difficulty for interested nurses to adjust schedules.
The combined barriers resulted in critically low enrollment in the first offering. The decision was made to proceed with the class despite the low enrollment due to the great deal of time and energy used while developing the program and since the use of grant money and CE hours was time sensitive. The decision to hold the class proved to be valuable because issues with the general processes such as wireless connectivity and handout materials were corrected prior to the next class offering that had an increased enrollment.
In addition to being proactive with alleviating potential technical difficulties, enough information had been gathered to create a checklist of processes and procedures for future classes. The checklist may be developed further to ensure that all specific policies and procedures are being considered. Nevertheless, the following five steps generally describe the processes that are needed to have a successful preceptor development program.
First, conduct a needs assessment of the facility or community in which the program will be initiated. If a preceptorship program is identified, then take a closer look at the objectives of the program before dismissing the idea to pursue a new course. As with the case of this program, often the design of preceptor programs focus on how to best integrate new nurses into practice rather than nursing students. If that is the case, then moving forward on the development of a new program or revising the existing program would be justified.
Second, solicit a team of educators and practice experts to collaborate on the course development. Consider including experts across practice areas so that the relevant concepts unique to the area, will be integrated. For example, new nurses have specific ongoing training and validation of skills which carries to the bedside for practice; it would be important for a preceptor to understand that although new nurses are trained to perform specific invasive tasks, students do not receive the same dedicated time and consequently delegating the task would be inappropriate.
The planning phase will be perhaps the most tedious process of the program development. It is at this stage that the newly formed team will need to agree on the most applicable course objectives, content that will be included, strategies that are needed to best meet the learning needs of the participants and the best person to teach content related to each objective. Because the course development may be a lengthy process, decisions about advertising for enrollment should be done concurrently. This will give sufficient notice of the upcoming program and will be beneficial in alleviating any scheduling conflict for potential participants. This parallel planning can be accomplished by dividing the group into subgroups with specific assignments to be carried out. In addition to course development, the planning phase should be the time in which the team determines financial needs, explores funding opportunities, and identifies associated budget constraints, if any. The team will also need to answer several procedured questions such as: How will participants get enrolled? How many participants will be in each course? Will there be prerequisites needed by each enrolled? What will be the charge for attendance, if any? Will a course reminder be sent to each enrolled? Will the course qualify to offer continuing education hours for completing the program? What will be the location of the course? What multimedia technology or other equipment will be needed?
The week prior to offering the first class session, the primary task for the team will be to ensure that everything discussed during the planning phase has been adequately addressed and completed. This would be a good time to make confirmation contacts to ensure the planned class location will be available with working equipment. If food and drinks were ordered, confirm timely delivery. Make certain that any requested printed materials will be available such as handouts and evaluation forms. On the day before the class, take a tour of the room location, check equipment, and become acclimated to the environment. On the day of the class arrive early, arrange seating as desired, have roster ready and greet each person upon arrival. The demonstration of greeting each one can be integrated into the class as a way of discussing how preceptors should be welcoming to the already nervous and sometimes fearful nursing students.
As with any implementation of a new program, it is essential to evaluate its effectiveness. Provide an evaluation tool at the end of the session to each participant. Gather the planning team to analyze the feedback and to also discuss what aspects went well and identify opportunities to improve from their perspectives. Use the information to make course revisions wherever applicable.
Building strong relationships and sustaining collaborative efforts between academia and clinical nurse educators can be invaluable to the success of preceptorship programs. The identification of a gap in adequate preparation of nurses to be effective preceptors for nursing students led to the creation of a workforce alliance aimed at developing an improvement plan. The alliance was between faculty within a baccalaureate nursing program and clinical nurse educators within an acute care facility. The primary purpose of the improvement project was to plan, develop, and implement a training program that focused on preparing baccalaureate level nurses to be effective preceptors for nursing students enrolled in BSN programs. The second aim was to provide staff nurses with a professional development opportunity by way of the preceptor training while earning continuing education hours.
Using resources gained through an internal grant, the group sets out to offer a program that would be different from most in that continued support would be given to the preceptor beyond the completion of class time. The innovative three-fold approach to a preceptor development program included face-to-face class time, supplemented with online learning, and followed with periodic on-site supportive visits by the program facilitators. Evaluative reports by participants indicated that the program was beneficial to their performance as preceptors. The facilitators believed that learning outcomes and goals of the program were well achieved. To determine statistical significance in the program's effectiveness, replication of the program is recommended with approval from the Institutional Review Board (IRB) to conduct a program evaluation research study.