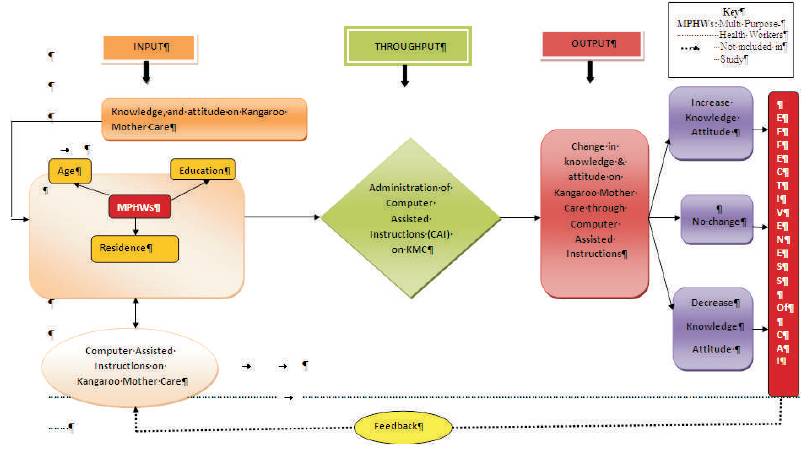
Figure 1. Conceptual Model Based on Ludwig Von Bertalanffy General System Theory
In India one third of all newborn infants are preterm and Low Birth Weights (LBW). Most of the newborn deaths are due to hypothermia and about 42 percent i.e, 3.6 million develop moderate to severe hypothermia. Kangaroo Mother Care (KMC) is a special way of caring of new born infants to foster their health and well being by promoting effective thermal control, breastfeeding, infection prevention and bonding. Multipurpose health workers (MPHWs) have a significant role in care of mother and child during prenatal, perinatal and postnatal period. Therefore, they need to have a vast knowledge and good attitude to deliver care to them. This paper tries to assess the effectiveness of Computer Assisted Instructions (CAI) in terms of gain in knowledge and attitude regarding KMC. A pretest and posttest control group with smple: 400 MPHWs, was used for the study. Six nursing Institutions of Punjab were selected conveniently and allocated to experiment and control groups (three institutes in each group) through stratified random sampling technique. The experiment group (n=200) were given teaching through CAI on KMC; control group (n=200) were getting standard teaching without CAI. After getting the permission from authority, the data was collected through pretested socio demographic profile data sheet, knowledge questionnaire and attitude scale. The data revealed that the knowledge of the subjects after CAI (experiment group) has improved significantly ('t'= 7.55, p<0.001) and control group had no significant difference in their pre and post knowledge score ('t'= 0.01, p>0.05). The pre test knowledge scores of experiment and control group had no difference ('t'= 0.01, p>0.05), but the post test scores of experiment and control group showed the significant difference in their knowledge scores ('t'= 5.84, p<0.001). There was also a highly significant improvement in attitude of experiment group (9.03, p<0.001) than control group. It was concluded that CAI is an effective teaching method to improve the knowledge and attitude of subjects than the tradition or routine method of teaching on KMC.
Low Birth Weight (LBW) among infants is a global as well an alarming problem in India. It imposes heavy burden on health care and social system almost on all the developing countries. India, with 1,220,200,000 (1.22 billion) people is the second most populous country in the world and represents almost 17.31% of the world's population. The birth rate (child births per 1,000 people per year) is 22.22 births/1,000 population (2009 est.) while death rate (deaths per 1000 individuals per year) is 6.4 deaths/1,000 population. Fertility rate is 2.72 children born/woman (NFHS- 3, 2008) and infant mortality rate is 30.15 deaths/1,000 live births (2009 estimated) (India Guide: Population of India 2013).
More than 20-million infants worldwide, representing 15.5% of all births are born with low birth weight, 95.6% of them are in developing countries and India alone accounts for 40 percent of LBWs in the developing world and more than half of those in Asia (UNICEF and WHO, 2004). According to WHO/UNICEF (2010), out of 26 million of total births in India, 0.94 million account for neonatal deaths. It is estimated that India contributes about a quarter of global neonatal deaths. More than 8.1 million newborns have low birth weight (less than 2.5 kg) and they have 30% chances of dying within the first 28 days of life as compared to normal birth weight babies. Among the LBWs, neonatal mortality rate is higher (91.4/per 1000 live birth) among very-smallsized babies.
The major contributors of death among LBWs are prematurity, infections, asphyxia, hypothermia and inadequate feeding. Hypothermia is one of the first and biggest problems among neonates. Existing evidences show that hypothermia contributes significantly to deaths of LBWs and pre term infants. Few data are available on incidence of hypothermia for home and institutional births WHO)estimates that 18% to 42% of worldwide annual infants' death is caused by neonatal hypothermia (Wariki, WHO 2010). The incidence of hypothermia has been estimated both among hospital and home born babies in low resource settings in South East Asia up to 85% (Kumar V, 2009) and north India 45% in normal newborns and 49% in LBWs (Darmstadt GL, 2006). Since the hypothermia during the newborn period is increasingly recognized as a major cause of neonatal morbidity and mortality. Adequate maintenance of thermo neutrality is important for the survival of newborn babies. The WHO recognizes newborn thermal care as a critical and essential component of essential newborn care. Half a million newborn deaths due to preterm complications can be prevented in each year if KMC were available to them especially in low socio economic countries ( Nagai S, 2010). Kangaroo mother (KMC) is a special way of caring of new born especially of low birth weight babies for effective thermal control. The concept was dated back from ancient time and its practice was first studied in Bogota, Columbia in 1978 by Dr. Reye and Hector Martinez as a result of a shortage of incubators in their hospitals. The significance of KMC was widely accepted and is now practiced in 25 developing countries of Asia, Africa and Latin America. It is estimated that more than 200 neonatal intensive care units practice kangaroo care today compared to less than 70 in the early 1990's.
KMC is inexpensive and does not need sophisticated equipment, can be applied almost anywhere to help to maintain normal body temperature. As we know in India about 75% of populations live in rural areas having less health resources and higher neonatal and infant mortality as compared to urban area. The smallest unit of health care delivery system in India is the sub centre which provides services to a population of 5000. The services provided by multipurpose health workers at sub-centre level. Though there is emphasis for the institutional deliveries, still the deliveries are being conducted at home. The care of mother and newborn is the responsibility of these skilled workers and they are in constant contact with mothers at the grass route level in the community. They need to practice various methods including KMC for management of hypothermia among normal and LBW newborns. Therefore they should have adequate knowledge and positive attitude towards KMC.
It is also observed that the MPHW students are taught through traditional lecture methods. Computer assisted instruction is an alternate to traditional instruction used both for on-campus and distance learning courses. A review of literature indicates that computer-assisted instruction (CAI) has a positive effect on student learning and attitude ( Calderone, 1994; Evans AE, et al 2000; Gaston, 1988). Hence in order to enhance the knowledge and attitude of MPHWs with CAI method regarding Kangaroo Mother Care, the present study has been undertaken with the following objectives:
Ho1: The mean post-test knowledge and attitude scores of o1 MPHWs of experimental group will significantly be higher than their mean pre-test scores.
Ho2: There will be no significant difference between pre and o2 post-test knowledge and attitude scores of MPHWs of control group regarding Kangaroo Mother Care.
Ho3: There will be no significant difference between post- o3 test knowledge and attitude scores of MPHWs under training of control and experimental groups regarding Kangaroo Mother Care.
Ho4: There will be no significant correlation between o4 knowledge and attitude regarding Kangaroo Mother Care among MPHWs of experimental and control group.
The conceptual framework of the study is based on 'General System Theory' by Ludwig Von Bertalanffy (1968). Systems theory views an organization as a complex set of dynamically intertwined and interconnected elements including inputs, processes, outputs feedback loops and the environment in which it operates and continuously interacts. The input in the present context is the computer assisted instructions which are used as the means to educate only MPHWs of the experiment group on KMC during the throughput phase. The expected change or improvement in knowledge and attitude of MPHWs is the output in this system. The feedback which is based on output is not included in the present study (Figure1).
Figure 1. Conceptual Model Based on Ludwig Von Bertalanffy General System Theory
A quasi experimental research approach with pretest posttest control group design was adopted for the study to assess the effectiveness of CAI on KMC .The study was carried out in selected six nursing institutions of Punjab. A multi stage sampling technique was used to select the sample. First of all six nursing institutions were selected conveniently and then a stratified random sampling technique was used to allocate nursing institutions into experiment and control group. The nursing institutions were divided into two strata: First stratum comprises of two institutions with intake of 80 MPHWs and 2nd stratum comprises of 4 institutions with intake of 60 MPHWs and then a non replacement lottery method was used to allocate of nursing institutions from each stratum into experiment and control group. Thereafter all the MPHWs of respective nursing institutions were taken as study subjects after meeting inclusion criteria. A total 200 subjects each in control group and experimental group were taken up for the study. The study subjects under experiment group were given teaching through Computer Assisted Instructions on Kangaroo Mother Care and the study subjects under control group were getting standard teaching without Computer Assisted Instructions on this topic.
Computer Assisted Instructions plan on various aspects of Kangaroo Mother Care (definition, components, indications, contraindications, benefits and procedure) was developed and checked for its validity by the experts in three point scale (meet the criteria=1; partially meet the criteria=2; does not meet the criteria=3) on its objectives, content, language, and presentation. Computer assisted instructions on KMC prepared in English was translated into Punjabi without changing the meaning and was validated by a Punjabi language expert.
A pilot study was conducted on 40 MPHWs to assess the practicability of the study and found feasible to conduct study.
Having received a formal permission from Principals of all selected nursing institutions, the class teachers were approached to get the attendance registers and time was taken for gathering the information from them. They were explained about the study and about all the activities to be carried out during the study and also assured for confidentiality. A written consent was obtained from them. After gathering the information on background of the subjects, a pre test was administered to assess their knowledge and attitude towards KMC. The experiment group was taught through Computer Assisted Instructions and control group had standard traditional teaching on KMC in a group of 30-40 separately. After 7 days a post test was administered.
The collected data was analyzed by using descriptive and inferential statistics. Calculations were carried out manually using a calculator and with the help of Microsoft Excel (2007). The statistical tests like mean, standard deviation were applied. In inferential statistics ANOVA;'t' test and chi square was used to compare the knowledge and attitude among control and experiment group during pre and post test and thereafter effectiveness of CAI was calculated.
Majority of subjects in both groups (experimental group 65. 5% and control group 50%) were in the age range of 21-30 years. The mean age of experimental and control group were 21.2±2.1 (range=17-25) and 20.7±2.1 (range=17- 26) years respectively. 120 (60 %) of experimental group and 108 (54 %) of control group resides in the rural area; 159 (79.5%) of experimental group and 150 (75%) of control group were unmarried; and 170 (85%) of experimental group and 159 (79.5%) of control group had no prior information about KMC. The data revealed that both experimental and control groups in respect to age (X2 value=6.47, df = 2), place of residence(X2 value=1.47, df = 1), marital status (X2 value=1.15, df = 1) and source of prior information (X2 value=4.27, df = 4) about KMC were homogenous (p>0.05). (Table 1)
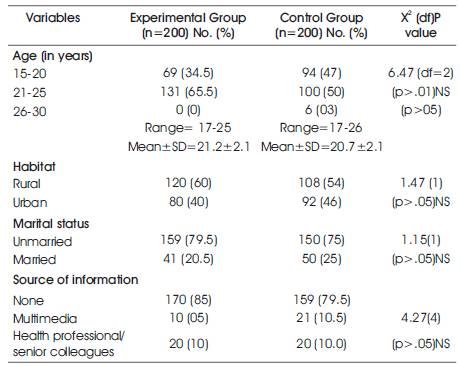
Table 1. Socio demographic profile of study subjects in experimental and control group (N=400)
The data revealed that the majority 160 (80%) of subjects in experimental group had below average knowledge and rest 40 (20%) had average knowledge in pretest and after the administration of computer assisted instructions, majority 151 (75.5%) had good knowledge followed by 39 (19.5) had average knowledge and 10 (5%) had excellent knowledge in posttest. Whereas in control group, majority 188 (94%) had below average knowledge scores followed by 12 (6%) had average knowledge in pretest and without intervention after 7 days followed by pretest, majority 141(70.5%) had below average knowledge followed by 59 (29.5%) had average knowledge in the posttest.
The pre test knowledge scores of experimental group was ranging between 10-16 with mean score 12.85±1.53 SD (mean %= 42.8) and posttest knowledge scores was ranging between 18-25 with mean score 21.56±1.98±SD (mean %= 71.9) and of control group was ranging between 8-15 with mean score of 11.45±1.80 SD (mean %= 38.2) and posttest knowledge scores was ranging between 8-17 with mean score 12.9± 2.16SD (mean %= 43.0). (Figure 2)
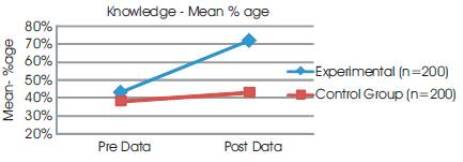
Figure 2. Mean percentage of pre test and post test knowledge scores of experimental and control group
On comparing pre and post test scores of individual group, the data shows a significant difference between pre and post test scores of experiment group ('t'= 7.55, p<0.001), and there is no significant difference between pre and post knowledge scores of control group ('t'= 0.01, p>0.05). While comparing the post test scores of experiment and control group, it shows the significant difference in their knowledge scores ('t'= 5.84, p<0.001) (Table 2).

Table 2. Mean pre-test and post-test knowledge scores of experimental and control group
Before CAI, 130 (65%) subjects of experimental group had unfavorable attitude followed by 70 (35%) who were undecided towards KMC. However, after the administration of computer assisted instructions 150 (75%) had favorable attitude followed by 50 (25%) who had highly favorable attitude towards KMC. Whereas in the control group 107 (53%) subjects had unfavorable attitude in pretest followed by 93 (46%) who were undecided and after 7 days on getting traditional teachings 106 (53.0) had undecided attitude followed by 94(47.0) who had unfavorable attitude regarding KMC. (Figure 3).
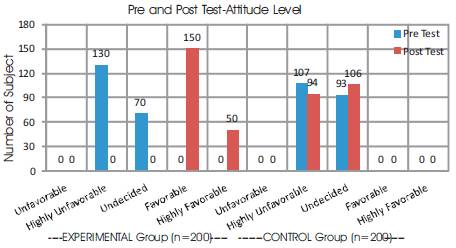
Figure 3. Pre and post test attitude level of experimental and control group
The data shows approximate 37% of improvement in the attitude scores of experiment group after the administration of CAI and found highly significant difference ('t'=9.03, p<0.001) between pre (mean ±SD=19.91±2.17) and posttest scores (mean ±SD=38.01±3.11). On the other hand there was a marginal increase (1.2%) in the attitude scores of control group and shows no significant difference ('t'= 0.001) between pre (mean ±SD=20.55 ±2.16) and posttest scores (mean ±SD=21.4±2.8). There is also a significant difference between post test scores of experimental and control group ('t'=4.35, p<0.001) (Table 3).

Table 3. Pre and post-test attitude scores of experimental and control group (N=400)
In experiment group, after the administration of CAI, the subjects revealed very high correlation of their knowledge with attitude (r=.96) and there was a negligible correlation between knowledge & attitude of control group (r=.03) on KMC. This means that as the knowledge improved after administration of CAI, the attitude of subjects towards Kangaroo Mother Care also improved (Figure 4).
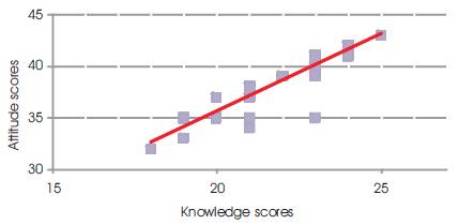
Figure 4. Scatter diagram showing correlation between post test knowledge and attitude scores of experimental group (n=200)
Computers have the potential to be useful tools to improve learning and a cost effective alternate to traditional teaching methods. In western countries, a great deal of research has been conducted regarding the effects of the use of computers as a teaching tool on student achievement, attitudes, learning rate, retention, etc ( Bloomfield J,2010; Fernandez Aleman JL, 2011; Ketsman, 2012). In Indian scenario, however, the studies in this topic are lacking. Is Computer Assisted Instruction (CAI) has the potential to bring about increased achievement in the Indian context when compare to traditional classroom teaching? Hence current study is an attempt to ascertain the effectiveness of Computer Assisted Instructions on Kangaroo Mother Care in terms of improvement in knowledge and attitude of MPHWs of selected nursing institutions of Punjab.
Of 200 subjects in experimental group 80% subjects had below average knowledge and rest 20% average knowledge in pre test but after receiving CAI on KMC 5% had excellent knowledge, 75.5% good knowledge and 19.5% average knowledge in posttest. Of 200 subjects in control group 94% had below average knowledge and rest 6% had average knowledge in pre test and after attending the routine traditional method of teaching 70.5% still had below average knowledge and 29.5% average knowledge in posttest (Table 2).
The data shows that the knowledge scores of group received CAI (21.56±1.98) was comparatively higher than the control group (12.9± 2.16) received traditional teaching (Figure 2). The average knowledge increased from baseline 42.8% to 71.9% and there was a significant difference between pre and post test scores of experiment group ('t'= 7.55, p<0.001) but control group did not show significant difference between pre and post knowledge scores ('t'= 0.01, p>0.05) in the control group and there was a marginal increase (3.8%) of knowledge score from baseline. On comparing the post test scores of experiment and control group revealed significant difference in their knowledge scores ('t'= 5.84, p<0.001) (Table 2).
A meta-analysis by Kulik, 2002 on 16 studies published since 1990 on the impact of CAI in mathematics in elementary and middle schools found slightly higher test scores and for nine of the studies the increase was statistically significant. A meta-analysis by Liao, 2007 on 52 studies comprising of 5000 subjects in Taiwan from first grade through college in English, physics, chemistry, statistics, mathematics and business found CAI had moderately positive effects on students' achievement over traditional instruction.
In the present study CAI is found to be effective teaching method when compared with control group receiving the traditional method of teaching to enhance the knowledge level of subjects on KMC (Table 2). A review of 59 research reports by Cotton, 1991 documented that CAI produced higher achievement than traditional instruction alone. The research study by Brothen and Wambach, 2000, on students receiving CAI on psychology course showed significantly higher pass rates and final exam scores than those receiving traditional instruction. Similar findings were also documented by Evans AE, et al 2000 that CAI group scored significantly higher on the scales measuring Auto Immune Deficiency Syndrome (AIDS) knowledge and other parameters as compared to 'lecture group' and also with 'no intervention group'. Rachelle N, 2009 found CAI effective to teach positioning and pushing guidelines during the second stage of labor than traditional classroom instruction as the CAI group showed a statistically significant difference (p < .05) in test scores immediately after instruction and 30 days post-intervention.
The literature documented that CAI is as effective as lecture method in terms of knowledge gain and retention for teaching nursing students on nursing research problem Gaston, 1988 and on fetal monitoring ( Murray and Higgins, 1996); about congenital heart disease as ( Rouse DP, 2000). ( Gega L, et al, 2007) also reported the same results while comparing traditional face-to-face teaching with computer-aided self-instructional programme on teaching pre-registration nursing students. Teal, 2008 found no significant differences in the test scores of pre-algebra students who received Computer Assisted Instruction (CAI) and Traditional Lecture (TL).
The data revealed that CAI is found to be more effective to improve the attitude level of MPHWs as compared to control group (Table 3) and a highly significant difference ('t'=9.03, p<0.001) was observed between pre and post test scores in CAI group and no significant difference ('t'=0.001 in control group. The studies conducted in abroad reported improved (Kulik and Kulik, 1986 and positive ( Gaston, 1988); Oermann MH, 1990) attitudes towards CAI as well negative (Brudenell I, Carpenter CS, 1990 ; and inconclusive (Calderone AB, 1994) towards CAI.
CAI on Kangaroo Mother Care was very effective as a teaching strategy that helped the MPHWs under training of selected Institutions of Punjab to improve their knowledge, attitude and comparatively better than traditional lecture method of teaching.
Based on the study findings, it is recommended that study can be replicated in different other institutions of nursing. Further studies can be carried out to teach diploma and degree nursing students and effectiveness of CAI can be compared with other teaching method alone and with combination of other teaching methods.