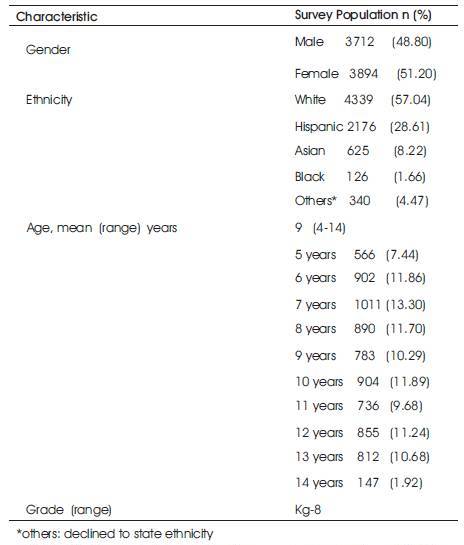
Table 1. Characteristics of the Survey population. ( n = 7606 )
The parents and the school district have been concerned about why children present to school nursing offices in elementary and middle schools. There is a limited amount of research that study these reasons. A retrospective survey study was conducted using the school nurses' visit logs from 7606 children. Minor trauma and abdominal pain were the most common reasons. A majority of students were returned to class, however a significant minority of 15.29% were excluded from school. Knowledge of the common reasons for presentation to school nursing offices is useful in preventing avoidable injuries and decreasing absence from school.
Health office personnel need to be aware of the common causes of morbidity in the school setting, so that care is optimized and appropriate preventive measures are instituted.
According to the American Academy of Pediatrics, the goals of a school health program in addition to others, is to provide a process for identification and resolution of student's health care needs that effect educational achievement (American Academy of Pediatrics 2001). The school nurse has a critical role within this school health program and provides acute, chronic, episodic and emergency health care.1 The National Association of school Nurses (2013) in a position statement, stated that students health and health needs must be addressed in schools to achieve optimum learning. According to the Centers for Disease Control (2006), the academic success of youth is strongly linked with their health. Thus helping students stay healthy is fundamental to the mission of schools.
Children present to school nursing clinic and health offices for a variety of reasons including illness, injury, behavioral or emotional issues, mental health problems and for routine
screening. The incidence of injuries and absences from school due to health problems continues to be linked with poor academic performance in the literature (American Academy of Pediatrics 2001). The purpose of this study is to verify and document the reasons for students coming to the school nurses office to seek for medical and other health related help. In the school health offices, the children are evaluated by a school nurse or a trained health technician. In the case of illness or injury, the child after evaluation may receive symptomatic treatment or first aid according to district policy and may be returned to class or excluded from school and referred to their doctor depending on the severity of the illness or injury. The importance of this study relies on the ability to identify and categorize types of injuries or ailments students are experiencing to institute preventive measures as well as to optimize care. It is important that school nurses and health personnel be aware of the common causes of morbidity in their populations and develop specific strategies to educate both the students and the parents.
Schneider et al (1995), reported that the common medical reasons for presentation to the school nurse are headache, infections, stomach aches and dizziness. However, this study was limited to high school adolescents. McKevitt et al (1977) in a paper titled, “Reasons for health office visits in an urban school district” reported that minor trauma was the complaint identified in the largest proportion of SHO visits at all levels from kindergarten through 12th grade. Taking prescribed medications was the second most frequent visit at the elementary school level (McKevitt et al 1977). Studies by VanArsdell et al (1972) and by Stephenson (1983) have specifically highlighted that elementary school child visits to the SHO, were mostly dealing with demographics and psycho social reasons for presentation.
The review of the literature pertaining specifically to elementary and middle school children shows a limited amount of research conducted on reasons for presentation due to illness or injury to the SHO during the past 20 years. The reasons for presentation to the school nurse clinic in younger children may be significantly different from that of older adolescents, both qualitatively and quantitatively. We decided to carry out a study to determine the health reasons why children in elementary and middle schools present to school health offices so that the school nurse working with the parents may reduce and prevent the health problems.
Design: A descriptive survey design was used to explore the incidences and categories of health care problems in kindergarten through eighth grade students, experiencing while they were in school. A retrospective chart review was conducted using 7606 cases.
The subjects were 9159 children enrolled in the Ocean View Public School District (OVSD) in Huntington Beach, California, during the 2010-2011 academic year. Of the 9159 children, 7606 came to the school nurse of illness or injury during the survey period (Survey Population). The school district has 11 elementary schools from Kindergarten through 5th grade and 4 middle schools from 6th through 8th grade. Subject inclusion criteria included all children who reported to the school nurses office for physical illness or injury.
The instrument consisted of a questionnaire that had two parts: Part I included demographic data such as child's age, gender, ethnicity, and grade level. Part II included a list of the following 14 categories of physical ailments: (i) Injuries, (ii) Abdominal pain, (iii) Headache, (iv) Nausea and vomiting, (v) Upper respirator y infection, (vi) Asthma/bronchitis, (vii) Insect bites, (viii) Non-traumatic pain, (ix) Conjunctivitis, (x) Earache (xi) Toothache, (xii) Skin rashes, (xiii) Epistaxis (xiv) Miscellaneous (fever, dizziness, child looking unwell, etc). The miscellaneous category captured data which included non specific fevers, dizziness and child looking or acting sick. Children who presented with symptoms such as cough, rhinorrhea and sore throat was classified as upper respiratory infections, pink eyes due to allergies or infections were classified as conjunctivitis. Viral exanthems, impetigo, eczema, allergic rashes and head lice were classified as skin rashes. Non traumatic pain included pain in the extremities, neck, chest and back not due to trauma. The scoring was done by counting the number of incidences in each category. Content validity was obtained by backing with the following literature (Chiou and Nurko 2011; Pennington 2010; Saps et al 2009; and Schnieder et al, 1995) Inter-rater reliability was obtained by having the PI and one of the school nurses score 10 of the randomly selected records and the agreement between the two scores was 95%.
Prior to starting data collection, permission was obtained from the School Board of the Ocean View School District and was deemed exempt from the District Institutional Review Board. The study is a retrospective analysis of school nurses visit logs of children attending the OVSD. All the schools had a School Health Office (SHO), staffed by either a school nurse (Registered Nurse) or a Health Technician. Prior to the commencement of the survey, the SHO personnel were trained by the principal investigator regarding the proper completion of the standardized health logs.
The logs were designed to capture the gender, age, ethnic group, grade, medical reasons for presentation to the SHO and the disposition of the child following evaluation. Only children presenting for illness or injury to the SHO were included in the analysis. Children who presented for non medical reasons such as emotional or behavioral problems, social issues, and normal physiological processes such as thirst, hunger and normal menstrual periods were excluded. Children who presented for routine screening for vision, hearing or scoliosis and for administration of prescribed medications, but were otherwise healthy were excluded. If a child presented with multiple symptoms the chief complaint was used in the classification. If a child presented multiple times in a single day for the same complaint, only the initial visit was included in the analysis.
Following an initial review of the health office visit logs, the chief complaints were classified into 14 categories which w ere in juries, abdominal pain , head ache, nausea/vomiting, upper respirator y infections, asthma/bronchitis, insect bites, non traumatic pain, conjunctivitis, ear ache, toothache, skin rash, epistaxis and miscellaneous reasons. The survey was conducted from September 9th 2010 through November 30th 2010. There were 53 school days during this period. During the academic year 2010-2011, there were 9159 children enrolled in the 11 elementary schools and 4 middle schools in the OVSD. The average daily attendance was 8965.
The data inclusive of the absolute numbers were entered into an Excel Spreadsheet. Data was then entered into statistical software (JMP Version 9 SAS Institute Inc.,) for further analysis. Descriptive analyses were used in terms of frequencies, means and percentages.
OVSD is a suburban school district that is ethnically mixed. It includes 11 elementary schools and 4 middle schools in kindergarten through 8th grade, with a student body of 9159. Of the 7606 children who presented to the SHO during the study period 48.80% were male and 51.20% were female. 57.04% were White, 28.61% Hispanic, 8.22% Asian, 1.66% African American and 4.47% were non classifiable. The mean age was 9 years with a range of 4-14 years. Results are presented in Table 1.
Table 1. Characteristics of the Survey population. ( n = 7606 )
With respect to the medical and health reasons why children came to seek help in the school nurses' office,results are presented in Table 2, showing that injuries accounted for 35.46% of presentations and were by far the commonest reason for presentation to the SHO. This validates prior research that has shown that injuries were the commonest reason for presentation to the SHO (McKevitt 1977). A study by Pennington (2010) stated that school injuries accounted for 10-25% of presentations to the SHO. However, both of the above studies were on children from kindergarten through high school. The significantly higher percentage of injuries in our study may be due to the fact that our survey was limited to younger children in elementary and middle school who may be more prone to injuries.
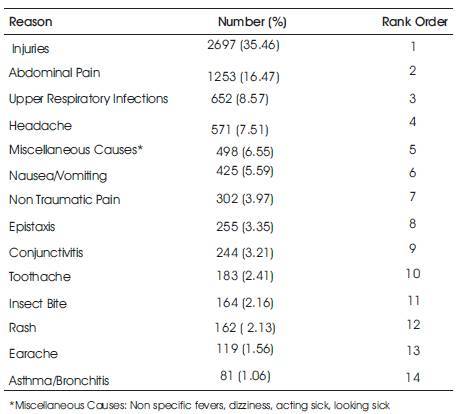
Table 2. Reasons for presentation ranked in order of frequency (n=7606 )
Abdominal pain was the second leading cause for presentation to the SHO in our population, that is 16.47% of the presentations. School based studies have reported that recurrent abdominal pain are common in childhood with 13-30% of children and adolescents experiencing abdominal pain weekly with up to 24% of children reporting symptoms persisting longer than 8 weeks Saps et al (2009) Hyams et al (1996). Youssef et al (2007) reported that recurrent abdominal pain effects up to 15% of school age children who face significant psychosocial consequences including school absences. Chiou and Nurko (2011) and Sprenger et al (2011) reported that the majority of recurrent abdominal pain in childhood are of functional etiology. Most of the abdominal pain in our population are probably also of functional etiology, however, this fact needs to be ascertained by further study.
Upper respiratory infections, headache, miscellaneous reasons (i.e., Non specific fevers, dizziness, acting or looking sick) nausea/vomiting, non traumatic pain, epistaxis and conjunctivitis ranked #3 through #9 and accounted for 38.75% of presentations. Toothaches, Insect bites, Rashes, Earaches and asthma/ bronchitis were the least common causes for presentation and ranked #10 through #14. They were less than 3% each and accounted for the balance 9.32% of the presentations.
The data show that in the majority of the children (84.71%) the illness and injuries were minor and they were returned to class to continue with their studies. However in a significant minority (15.29%) the illness or injuries were severe enough for the child to be excluded from school and either to be sent home or referred to their doctor for further evaluation. Thus, the specific reasons for exclusion from school and whether it is justified merits further study.
According to the American Academy of Pediatrics (2008), one of the core roles of a school nurse is to provide care for injuries and acute illness for all students. The point of first contact for an injured or ill child is the school health office, where the child is evaluated by the school health office personnel and the decision is made to return the child to class or to exclude the child from school. It is therefore appropriate that SHO personnel are aware of the common causes of morbidity in the school setting so that the children may be appropriately evaluated and treated.
Knowledge of the common causes of morbidity in elementary and middle school children in the school setting is useful in planning education programs for SHO personnel, so that they can be better prepared to educate, evaluate and treat children presenting to the SHO.
The high incidence of injuries in this population makes it important to institute and reinforce injury prevention measures in order to decrease avoidable injuries. Further research on school-related injuries should be done to add to the body of literature and would have important implications for the children, parents and school nurses.
Though the SHO visit logs were standardized, input biases cannot be excluded in filling of the health logs, since there were health office personnel (i.e., Registered Nurses and Health Technicians) with different levels of training and experience.
Results are based on one school district. Hence caution should be exercised in generalizing to other school districts. OVSD is a suburban school district that is ethnically mixed. Hence whether the results are applicable to urban or rural school districts or to school districts with more homogeneous populations need to be ascertained by further study.
According to this study, in elementary and middle school children, injuries, abdominal pain, upper respiratory infections, headaches, miscellaneous reasons and nausea/vomiting were the common reasons for presentation to the school health office. Though most of the presentations were benign, a significant minority were severe enough to be excluded from school.
In order to institute preventive measures and optimize care, it is important that SHO personnel be aware of the common causes of morbidity in the school setting.