Figure 1. Ruland, C. M., & Moore, S. M. (1998). Theory construction based on standards of care: A proposed theory of the peaceful end of life. Nursing Outlook, 46(4), 174
Providing appropriate end-of-life care has become a primary concern of nurses. In today's world, it is important for nurses to strengthen their knowledge regarding end-of-life especially for elder people. The purpose of this article is to study the theoretical underpinning, concepts, metaparadigms and definitions of the peaceful end-of-life framework proposed by Cornelia Ruland & Shirley Moore in 1998. Proposed theory was reviewed in depth to identify the concepts emerging from end-of-life care. Ruland & Moore have defined five major outcome standards that contribute to a peaceful EOL for terminally ill patients. (1). being free from pain, (2) experiencing comfort (3), experiencing dignity and respect, (4) being at peace and (5) experiencing a closeness to significant others or other caring person. This theory contributes the rich body of knowledge for nurses the need to provide end-of-life care. It provides insights and can contribute to increase knowledge about nursing interventions that provides peaceful end of life to the terminal ill patients.
Since past years, the development of middle range theories has been increased. Recognition of these theories in the nursing field provides knowledge and has been stimulated to address issues related to clinical nursing practice (Ruland & Moore, 1998). Middle range theories are applied and can be tested in clinical situations. These theories offers framework which provide guidance for nursing interventions. Several Middle range theories (Maternal role attainment, uncertainty in illness, self transcendence theory, theory of chronic sorrow, theory of comfort, theory of caring and peaceful end of life theory) have emerged in the literature and can increasingly applied and tested at various clinical settings (Tomey & Alligood, 2010). These theories provides specific framework which provide guidance to the nursing interventions in daily day clinical practice guidelines. Nurses emphasize physical interventions as an integral part of their clinical process; however majority of the nurses did not feel comfortable discussing end of life care with the patients (Murrish, 2010). So, in order to provide appropriate end-of life care, it is important to study the literature addressing end-of- life care.
The aim of this paper is to discuss the use of Ruland and Moore: Peaceful end of life (EOL) from middle range theory for the care of older patient.
Cornelia M. Ruland, received Ph.D in nursing degree from Western Reserve University, Ohio, in 1998. She has been primary investigator of number of research projects, having extensive experience on various research programs in improving patient-provider partnership in health care (Tomey & Alligood, 2010). Also, Shirley M. Moore, received her Ph.D in nursing science in 1993. She has gained experience in teaching nursing theory and nursing science subjects to nursing students. She conducts various research programs at graduate and undergraduate level studies. This theory was derived during the doctoral theory course in which Moore was the faculty and Ruland was the student. Ruland was able to successfully complete the project and developed standard clinical guidelines for the peaceful EOL (Tomey & Alligood, 2010).
The End of Life (EOL) theory is based primarily on the classic work of Donabedian's Model, which consists of standards includes structure, process, and outcomes. In this theory, structure is the family and terminally ill patient that are receiving care from health care professionals, process defined as those nursing action which are intended to endorse the positive patient care which results in positive outcomes in clinical settings. There are several middle range theories that address the aspects of EOL care, however none of the nursing theories exists which provides framework that consist of all the aspects that are necessary for the terminally ill patients. The need for this theory was identified when there were no formal clinical guidelines. “The lack of clearly defined directions for terminally ill patients, serves as barrier for provision of quality nursing care (Ruland & Moore, 1998, p.3)”.
The development of this theory resulted in initiation of new standards for the patient about peaceful EOL. Ruland & Moore (1998) cited “The main focus for the development was not dying itself; but contribution to peaceful and meaningful living that remained for the patients and their significant others (p.171)”.In nursing homes; many patients are in EOL stage, facing problems of all dimensions and need comfort care. They have several discomfort feelings (nausea, thirst, elimination problem and other bodily related problems which they were unable to verbalize and ventilated (Ruland & Moore, 1998).These concepts were not entertained. At that point of time, they need physical, social as well as psychological care.
This theory provides a new dimension that will enhance and provide best possible nursing care for the terminally ill patients. Another very important point is that the terminally ill patients are not able to communicate their pains, distress, and sorrows to the nurse who are involving in their care. Therefore, it is important for nurses to make patient rest of the life in meaningful manner.
Ruland and Moore (1998) addressed meta paradigm concepts to provide holistic peaceful EOL. These were nursing, person, environment and health. They have identified two assumptions in this theory. Firstly, the feelings at EOL experience are personal, are based on individualized patients and secondly nursing reflection on dying patient interventions. The goal of EOL care in not to optimize care in terms of technological or over treatment rather the primary goal is to provide best possible comfort measures in order to achieve quality of life and peaceful death (Patricia in Alligood & Tomey, 2010 p. 756-757). Ruland & Moore theory was straight forward and clearly progressed. It was widely practiced over community development as a means to improve EOL decision making for critically ill adults, integrated into nursing courses and for research purpose (Patricia in Alligood & Tomey, 2010 p.757). The concept of hospice and palliative derives from Ruland & Moore's.
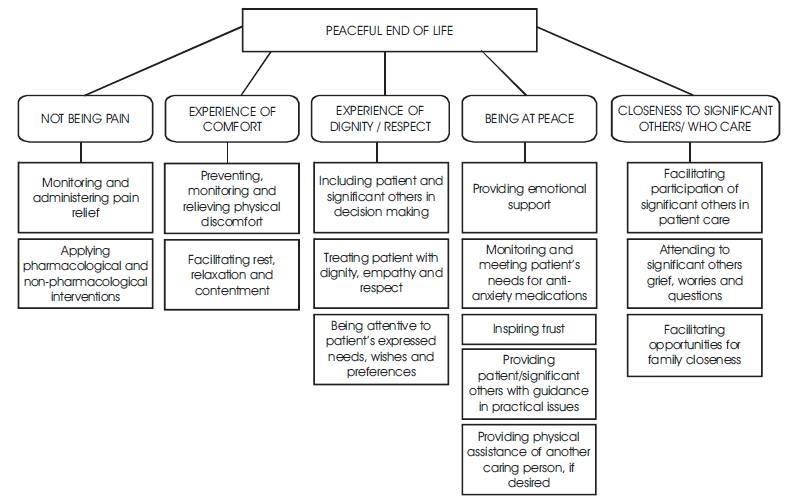
This theory on EOL was proposed from direct experience of nurses who had 5 years of clinical experience and thorough literature review. This theory attempted to clearly described, observable concepts that express the idea of caring (Patricia in Alligood & Tomey, 2010, p. 756). Ruland & Moore (1998) defined five outcome standards that contribute to a peaceful EOL for terminally ill patients. (1). being free from pain, (2) experiencing comfort (3), experiencing dignity and respect, (4) being at peace and (5) experiencing a closeness to significant others or other caring person (p.174). The conceptual definition of outcomes standards were thoroughly and well defined in the several literatures. To visualize the relationship between five standards of EOL care for terminally ill patients, see Figure 1.
Figure 1. Ruland, C. M., & Moore, S. M. (1998). Theory construction based on standards of care: A proposed theory of the peaceful end of life. Nursing Outlook, 46(4), 174
Firstly, being free from pain means not having any sort of pain. Pain is unpleasant, sensory experience which is associated with any actual or potential tissue damage (Patricia in Alligood & Tomey, 2010, p. 780). Almost in many literatures, pain has been well defined including its assessment, management and treatments.
Secondly, experience of Comfort was defined as “Relief from discomfort, the state of ease and peaceful contentment and whatever makes life easy or pleasurable (Ruland & Moore 1998, p.172)”. In nursing homes, most of the patients were sick, bedridden and terminally ill. They were in the state of discomfort and it could be due to many reasons (e.g. nausea, thirst and elimination problem). Ruland & Moore (1998) described few actions that help patients experience comfort. It includes providing comfortable bed position, preventing from bed sore, using therapeutic touch, offer comfortable activities like music, massage, physical activity, mouth care, foot care and eye care (Ruland & Moore, 1998, p.173).These theorists very nicely identified three criteria to facilitate patient comfort: (1) Preventing, monitoring and relieving physical discomfort, (2) facilitating relaxation and (3) preventing complications (Patricia in Alligood & Tomey, 2010 (Figure 1).
Thirdly, experience of dignity/respect is another third very important indicator for terminally ill patients. Every human being liked to be respected and valued. For a terminally ill patient, it is important that they should be include in decision making, treat them with dignity, empathy and respect.
Fourthly, being at peace involves the sense of serenity, calmness, harmony and contentment. It is suggested that patient should be free from all sort of worries, anxieties, and fear. This can only be done by providing emotional support, by meeting the needs for antianxiety, by inspiring trust, and by providing physical assistance if desired.
Finally, experiencing the closeness by providing the feeling of connectedness to other significant persons. It can also be achieved by facilitating opportunities to meet and share with their close family members.
The application of these theories provides guidance that lead to positive interventions. The rationale for selecting these theories was that it was relatively simple, logical in nature, generalized, understandable and facilitates nurses to improve their clinical practice. It explains about quality of life and delivers significant concept in EOL in research and practices both. This is the best approach to deal with EOL patients.
Caring is the essence of nursing and disciplinary foundation core of profession (Watson 1985/2008, p.17). In nursing profession, we are always talking about caring concepts, to care people around us, helping trusting relationships and to have peaceful death for our patients who are terminally ill and so on. However, in reality somehow we miss all those concepts of caring. We would love to work on fancy and attractive projects but the essence of 'real nursing' is lost somewhere in between.
The development of this theory is very significant because it can guide nurse in selecting interventions that alleviate suffering and help patient lives a meaningful experience. All those patients who are terminally ill are going through the terrible feeling of fear and worry. At that point of time, nurses plays key role in providing compassionate care at this stage. The development of this theory provides a unique way to care for terminally ill patient and can contribute towards effective nursing interventions. With the application of this theory, nurse will able to identify the ways to prevent patients from unnecessary suffering and to maintain dignity and respect.