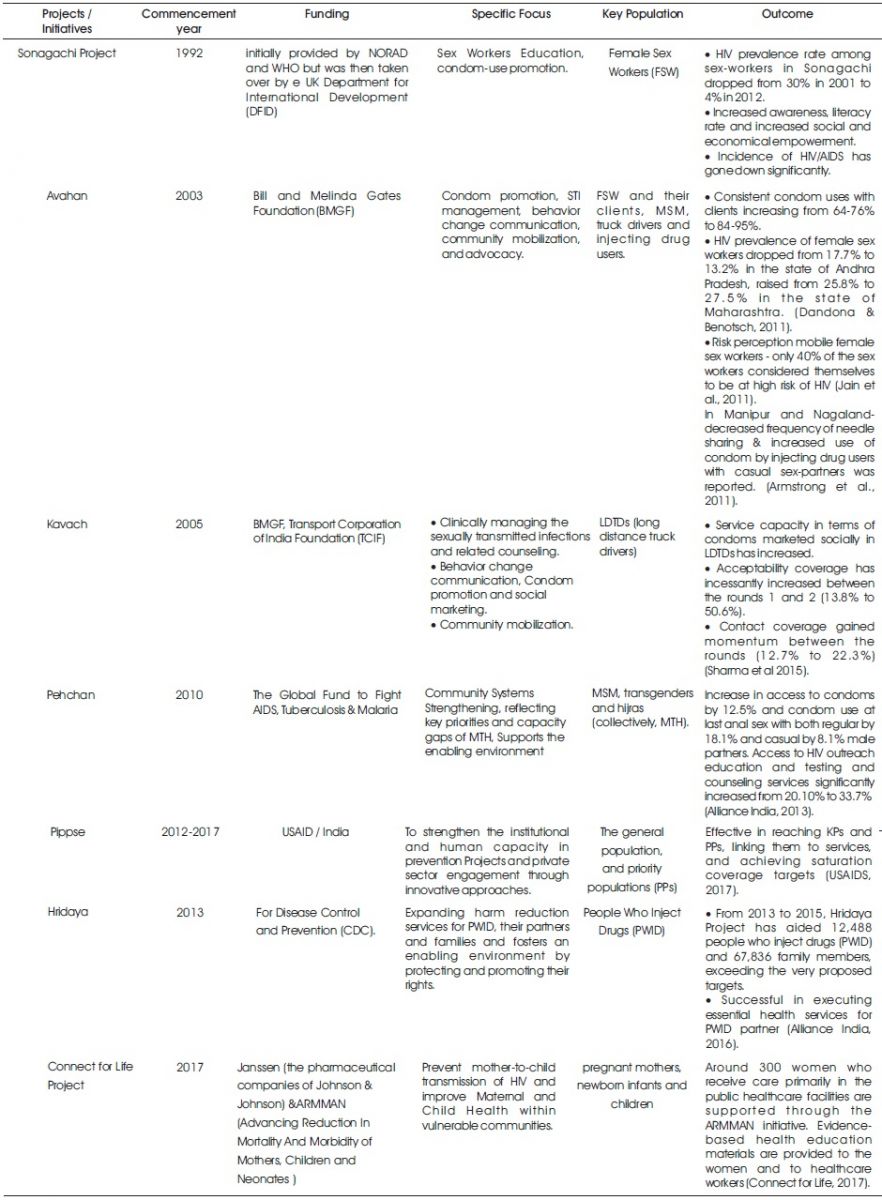
Table 1. Successful Projects on HIV Prevention
The first AIDS case in India was reported in 1986, and as the epidemic was spreading, there was a need for nationwide efforts. Over time several successful Projects have been operated to control the epidemic. HIV Projects have successfully evolved over a timeline of last 25 years. This paper attempts to review a few such projects to assess their evolution with time and to evaluate their impact to guide other disease intervention projects for other infectious epidemics, especially in Tuberculosis (TB) and HIV TB co-infections. Effective evaluation of these projects has provided the evidence based foundation for projects over time. The methodology used for the analysis of projects was done through an exhaustive literature search, from peer-reviewed articles and international/national and Government/Non-Government Organizations' (NGO) reports. These projects have previously been successful in increasing awareness, literacy rate and effecting socio- economic empowerment of the key population. Assessing these projects has provided the best practices and approaches as key learning as compiled in this paper. Taking lessons from the HIV–AIDS projects and applying them in other projects could shorten the learning curve for other disease prevention and control.
There are 2.1 million people living with HIV in India, with 0.3% adult prevalence, 80,000 new infections, 62,000 AIDS related deaths, 50% adults on antiretroviral therapy and 33% children on antiretroviral therapy as recent as 2016 (Joint United Nations Project on HIV/AIDS, 2017). India's first National AIDS Control Programme (NACP) was launched in 1992, and National AIDS Control Organization (NACO) as a division the Ministry of Health and Family Welfare (MoHFW) was constituted to provide leadership to HIV/AIDS control Project.
Over time, the focus has shifted from raising awareness on behavior change, from a national response to a more decentralized response and to increasing involvement of NGOs and networks of people living with HIV (PLHIV).
The key populations (KP) most affected by HIV in India are:
A growing evidence base has enabled the government and stakeholders to mount a well-informed and sharpened national HIV response. Various Projects have been undertaken in India to address the epidemic. A well planned and carefully executed evaluation reaps more benefits for all stakeholders.
Evaluation of Projects helps us to know:
This paper documents a comprehensive analysis on reduction of HIV/AIDS among the population being served, by analyzing various anti-HIV Project that will aid in producing best-practices on conducting community-wide various disease reduction and awareness interventions.
An exhaustive literature search of peer-reviewed articles, International/national and Government and Non-Government Organizations' (NGO) reports was conducted.
Inclusion Criteria: Major HIV Projects that have evolved over the timeline of last 25 years and that are multiyear projects with large funding and having availability of individual evaluation reports in the public domain. Selection of the projects was done keeping in mind the variety of key population targeted by these projects.
The methodologies of the evaluations used within various projects combined numerous instruments, such as analysis of documents, focus group discussions, in-depth interviews, group meetings, a review of project documents, media reports, police record, pre- and post-intervention cross-sectional survey design with retrospective analysis of programmed data reports review and mixed methods study, with key informant interviews.
Various HIV–AIDS projects have taught us the value of societal engagement: successful projects have actively drawn in the affected communities, stigma reduction, energized advocacy, and political support and will. These Projects have reflected that building the evidence for what works where, and for whom, in combination of HIV prevention strategies can guide the Project Managers, not only in designing projects but also in selecting appropriate methods to evaluate and constantly improving them. Table 1 below depicts a few of such successful projects which have been further discussed in detail.
Table 1. Successful Projects on HIV Prevention
Illustrating further, In Sonagachi project a distinctive method of engaging sex-workers to be peer educators who train other sex-workers all about safe-sex practices was adopted, which became the role model for sex-workers in other parts of the world to fight socio-economic health disparities. It involved participation based communication intervention at the community (re-defining the problem), group (peer outreach) and individual (empowering sex workers) level. The positive experiences from Sonagachi Project were inspiring and were used to guide Avahan Project in the design phase (Jana et al., 2004). It was sound prevention planning, considering the dynamics of local epidemic, the target populations in their context, the evidence base and “lessons learned from other projects”. And the intention was “learn as we go” (Laga & Vuylsteke, 2011).
Avahan should be commended for making learning by evaluation a crucial part of its effort. Avahan's evaluation design did not include the community mobilization from the start but later included community mobilization. Avahan in its very foundation, recognized that creating an enabling environment while working with the highly stigmatized and marginalized populations was indeed essential for project improvement.
Avahan's prospective and intended evaluation design incorporated at least two consecutive surveys, Integrated Behavior and Biologic Assessments (IBBA), various district population surveys, monitoring of project execution data and intervention uptake, also the cost analysis.
The project provided key evidence to NACO on the significance of community mobilization in HIV prevention intervention. Peer-led outreach and community mobilization approaches, cutting across all projects, were vital to Avahan's design. During Avahan's mid-term evaluation, Intervention Design of LDTD Project was refined.
The Avahan partner, TCIF, initially set up intervention sites at 36 locations by the sides of the major national highways. However, the project data indicated that despite a national presence, critical project gaps remained. A behavior-tracking survey in mid-2005 unfolded that project awareness was merely 12 percent and the service uptake was 7 percent. In response the project decided to: Focus interventions on the major impact locations & intelligent placement of services. These changes resulted in doubling of monthly communication reach and monthly clinic uptake as well as a 50 percent increase in monthly condom sales.
Another Project which emphasizes the importance of community involvement, provided the substantial evidence towards it; is Pehchan Project. The community-based, client-centric and gender-affirming methods exercised by it significantly raised the demand for and access to tailored health, HIV, psychological, social and legal services for the transgender people. Community participation and collectivization approaches reinforced self &collective efficacy of transgender communities and empowered them. Furthermore, structural changes in the legislative framework to decriminalize and legitimize sexual practices among transgender people were a priority (Shaikh et al., 2016).
Moving further, with community centric approaches such as peer counsellors involvement and mentorship, the Hridaya Project aims to increase community mobilisation and provide site specific support to harm reduction and HIV prevention strategies which have been extremely effective in bringing about substantial increase in the uptake of services and Female Outreach Workers (FORW) to address the issues related to spouses/regular sex partners of PWID and shown positive result. NACO included FORW in NACP IV after seeing the evidence of the importance of reaching out to spouses and partners of male PWID in national HIV Projects (Alliance India, 2016).
HIV Projects have impressively focused on the needed approaches for further improvement. Of such approach one project called PIPPSE (Impact through Prevention, Private Sector and Evidence-based Programming) to strengthen the institutional and human capacity in prevention projects and private sector engagements through innovative approaches to contribute to achieving the goal of accelerating the reversal of HIV epidemic. Two components of the project are: Social Protection and Financial Inclusion, National AIDS Helpline.
In PIPSE project District Network Model (DNM) approach was found to be effective in reaching KPs and PPs, linking them to services, and achieving saturation coverage targets.
Prevention of Parent-To-Child Transmission Project in India (PPTCT) and free ART Projects have made a laudable effort in reaching out to a huge number of HIV-infected women and their children. Incorporating unique approach Connect for Life Project supports the development of m- Maitri, an initiative to educate pregnant women on techniques to prevent mother-to-child HIV transmission. At the initial stage of their pregnancy, women receive tailored voice messages to their mobile phones imparting the general advice and support on pregnancy as well as peculiar information related to being pregnant and while HIV positive (Connect for Life, 2017).
Good surveillance systems for diseases and their risk factors are crucial for measuring the magnitude of the problem and its associated costs, identifying vulnerable subgroups, and evaluating the effects of policy and practice interventions.
“We have moved from despair to hope, from denial to acceptance, from stigma to reduction in stigma, from a death sentence to a chronic manageable disease and should now aim for donor funded to domestic funded project and standalone to more integrated projects". (Rewari, 2013).
The battle against HIV/AIDS is an excellent example of coordination between government and non-government agencies, diligence, dedication and scientific innovation. Figure 1 presents the key learnings.

Figure 1. Key Learnings
A comprehensive inclusiveness and how various HIV Prevention & Control Projects were successful in disease control and raising the awareness, aided in identifying the key factors that are essential to create a significant impact. Learning these lessons from the HIV–AIDS projects and deploying them in future Projects would improve the learning curve for other diseases prevention and control.