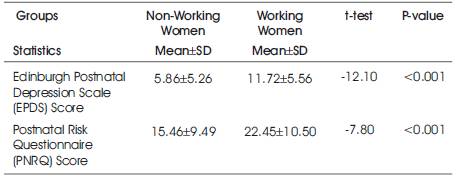
Table 1. Comparison of mean EPDS and PNRQ between non-working and working women
Parenthood is a transition period, characterized by significant change in a new parent's life, which is called post-partum period. It's a time in which woman undergoes the transition of motherhood to parenthood. It is extremely important to manage the postpartum period very effective if not, then mother may go through postpartum depression stage. The Cross Sectional Study design was used to determine whether there is a difference in the rate of PPD between working and non-working mothers as well to determine whether there is a relationship of associated factors of postpartum depression among working and non-working women. The data were collected using the validated EPDS & PNRQ Tool and a General Questionnaire. A Chi square test was used to determine the difference in the rate of PPD between both working and non-working mothers during the postpartum phase. According to Edinburgh postnatal depression scale, no depression was found in 202 participants of non-working women (80.8%) whereas in working women only 89 participants reported no depression (35.6%) and this difference was found to be statistically significant at P<0.001. The study findings revealed that there is increase in postpartum depression in working mothers than non-working mothers; therefore, early intervention could be planned in the form of group teaching sessions which will help new mothers to develop a friendship network to support with the challenges of caring for her preterm infant.
Stress is a multidimensional phenomenon and many studies indicate that working women have many types of stress in their life. Postpartum depression (PPD) is a significant health issue which affects the women’s mental health after child birth. It includes loss of concentration, sleep disturbances, loss of energy towards daily life activities and feeling of fatigue. Its negative effects remain from 4-6 weeks after child birth. Postpartum depression (PPD) is a serious issue due to its distressing effects on the mother, family, and children. The prevalence of PPD among Pakistani women varies from 28 to 33% (Muneeret al, 2009). Various studies on PPD have identified several environmental, social, and cultural risk factors. The common risk factors in Pakistani women are economic deprivation, poor relationship with the husband, female infant gender, increased number of children and illiteracy (Hussain et al, 2000).
The Objective of the study is to determine postpartum depression among working and non-working mothers living in the general population of Karachi, Pakistan and determine associated risk factors for postpartum depression among working and non-working mothers and to identify if there is any association of parenting stress, interaction between mother and infant with postpartum depression among Pakistani working and non-working mothers.
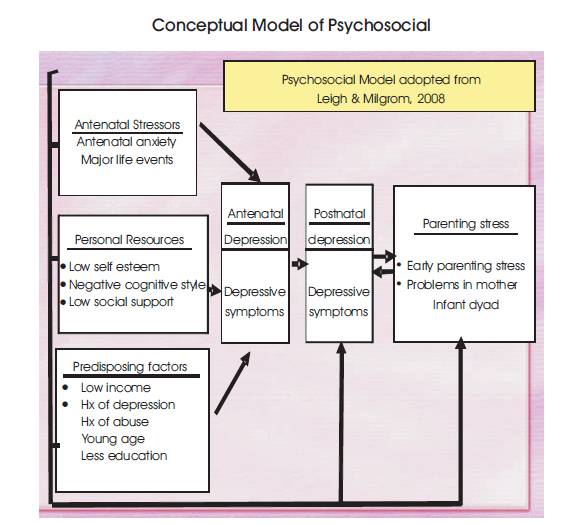
The literature review has three sections. The first section describes the Leigh and Milgrom (2008) framework (refer Annexure 3) which guided the literature review and the study. The second section focuses on postpartum depression and its prevalence worldwide. The third section discusses contributing factors to the development of PPD.
The framework which guided the literature review and the study is the 'Psychosocial Model' of Leigh and Milgrom (2008) (refer Annexure 3). This model comprises of four components which includes antenatal depression, postnatal depression, Parenting stress and Risk factors associated with mental health. According to the model, mothers can develop depression during pregnancy or after delivery or during both time periods (Leigh & Milgrom). PPD is defined as the feeling of sadness and anxiety which could affect the functioning of mothers in daily life after delivery (Santrock, 2007). Mothers suffering from PPD show significant parenting stress. The stress pertaining to parental stress is “disparity between the demands associated with parenting role and the perceived availability of resources for dealing with those demands” (Misri, Reebye, Milis, & Shah, 2006). Early parenting stress could be defined as stress related to characteristic pertinent to the parents, infants, and situations which directly affect parental role. Mother infant interaction is a “process of bidirectional mother infant attachment (infant attachment and maternal bonding)” (Kashiwagi & Shirataki, 1995). Due to PPD mothers may develop early parenting stress or due to early parenting stress, mothers may develop PPD.
The risk factors are divided into three categories: antenatal stressors, personal resources and predisposing factors; however this study only focuses on predisposing factors. Predisposing factors include history of abuse, history of past psychiatric illness, age, low income and low education, it has negative implications on mother infant interaction and of parental stress. According to the model all these factors could add to parental stress and lead to PPD and create parental stress. Hence, predisposing factors of PPD and parental stress consequently are potential confounders in this study. In the proposed study predisposing factors will be measured to identify the relationship of predisposing factors with PPD and parenting stress.
It is estimated that 150 million people undergo PPD, which leads to morbidities due to depression, and annually, there are nearly 1 million commit suicidal attempts. There were lot of global research studies which showed that although the life expectancy of females is more than males, it is not necessary that they live better or healthier than their counterparts due to their specific mental health problem, leading to depressive disorders are more prevalent in females 41.9% as compared to 29.3% in males (Zahidie et al, 2011).
Postpartum depression is higher in non-working women than working women. The study indicated higher levels of depression due to lack of social interaction, compromised marital status, Lack of social and family support and less confidence to face the challenges of life. Social and family support variation in nuclear and extended family system, and related study revealed that there was higher depression in women in the nuclear family system due to high levels of stress due to increased tasks (Gurudatt, 2014).
Rada et al in 2011 studied the effects of workload with other work-related factors for postpartum depression in working mothers in the initial 6 months after childbirth. The study showed higher depression with those who have high workload, lower job flexibility, and low social/family support, an infant with disturbed sleep patterns and issues with breastfeeding. Author concluded that working mothers of postnatal phase should have flexible duty hours in order to manage their infants and need quality time with peace of mind.
There may be many factors which include poverty, more children, uneducated husband, lack of friends, life events, and social support. Whereas, in a hospital setting unwanted pregnancy, primipara pregnancy, living in extended family, marital difficulties, past experience of infant death were identified as the risk factors which are different from rural areas (Kalyani et al.2001). On the other hand, in peri-urban areas the identified risk factors were domestic violence, difficulty in breastfeeding, and unplanned pregnancy (Ali et al.2009). Hence, predisposing factors for PPD are variable and differ depending on the area/setting. Mothers with a history of abuse are at a higher risk of developing PPD, which results in disturbance in mother-infant interaction. Low socioeconomic status is also a risk factor for PPD. Studies show that mothers with economic difficulties (Klainin & Arthur) and poverty (Rahman & Creed) are at greater risk for developing PPD. Moreover, when mothers are unemployed, parental stress is high. Husband's education may contribute to the development of PPD in mothers (Beck, 2001;Rahman & Creed, 2007;Rahman et al., 2003). (Inandi et al. (2002) reported that a woman, whose husband is uneducated is 1.7 times at greater risk of developing PPD than a woman whose husband is educated. Mothers' age (Rahman & Creed, 2007) may contribute to the development of PPD. Mothers with young age have a lower risk of PPD than mothers with older age (greater than or equal to 30 years). Their study highlighted that non adolescent mothers show more positive affect towards their infants. Mothers lacking social support tend to face difficulty in completing their household chores. A study was conducted between postpartum mothers of two groups, the one who gave birth to female child and another group who gave birth to the male child. The study revealed that birth of female child increases the likelihood of postnatal depression as compared to male child due to cultural factors. (Mirrat, Saqib & Saima, 2013). Neece and Baker (2008) reported increased level of parental stress in mothers of disabled children, congenital abnormalities or deformities (e.g., Down syndrome, a congenital heart defect or cleft lip or palate) or chronic illness. Therefore, mothers with still birth or whose infants have congenital abnormalities will be excluded from the study to better understand the relationship between disease process and PPD.
The cross sectional Study design was used to determine whether there is a difference in the rate of PPD between working and non-working mothers as well as to determine whether there is a relationship of associated factors of postpartum depression among working and non-working women.
The study setting was mothers from 6 weeks to 12 months of the postpartum period from general population.
Postnatal mothers who delivered baby within one year of the time period.
A sample size of 500 mothers (250 each for working and non-working group of postpartum mothers) were calculated based on a G power sampling calculator with a 5% margin of error.
A non-probability sampling approach, which is purposive sampling technique was used.
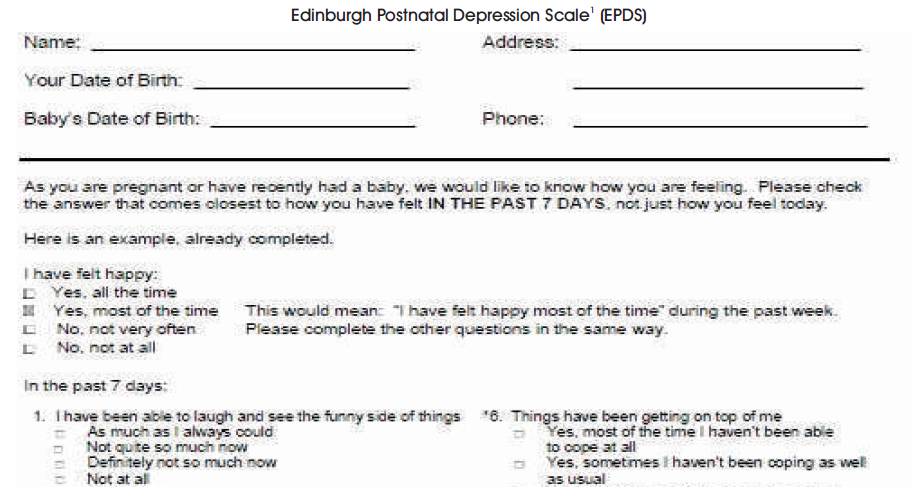
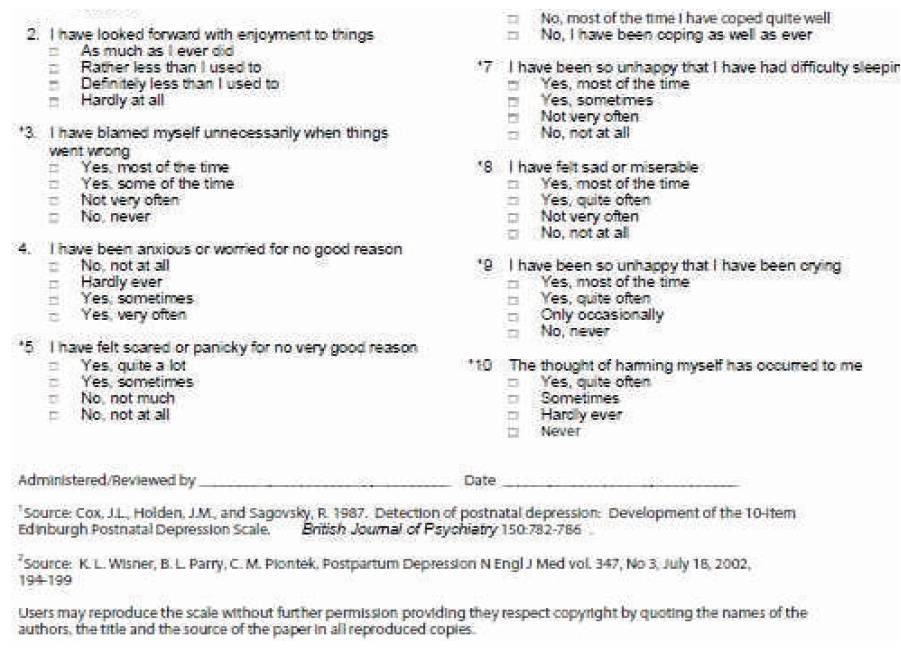
The Edinburgh Postnatal Depression Scale, EPDS (Refer Annexure 1) was used. EPDS is a 10 item questionnaire asking about the depressive symptoms. The tool is tested for its reliability and validity. The minimum is 0 and the maximum total score is 30. Mothers who score 12 and more are likely to be suffering from PPD. It takes only five to seven minutes to complete the questions.
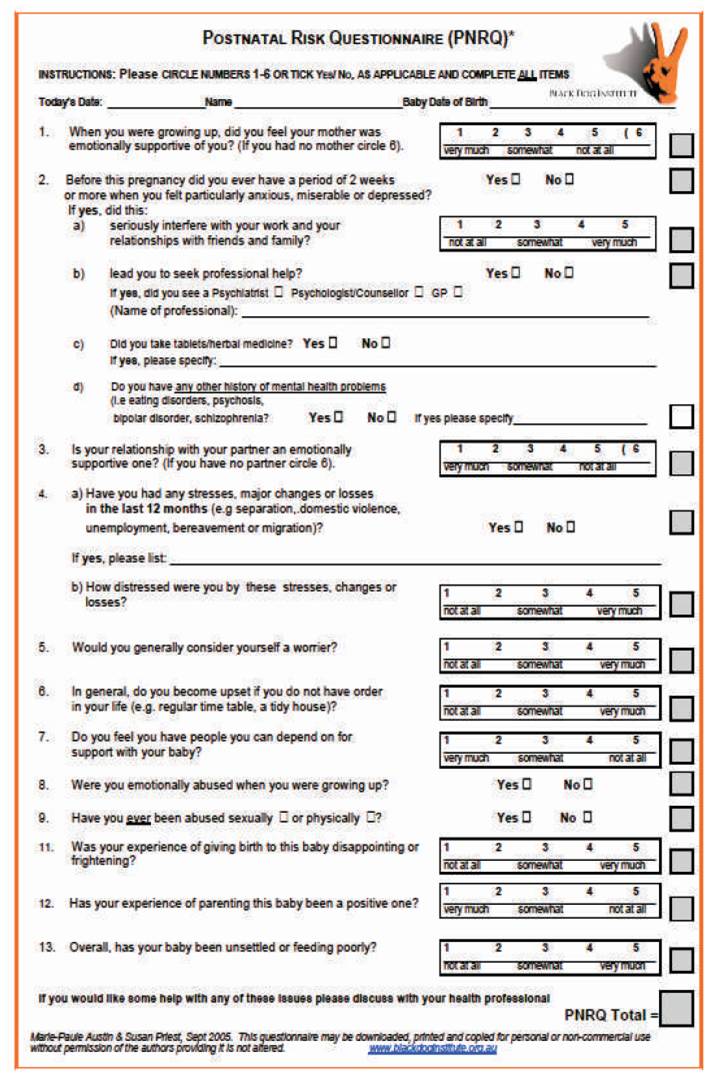
Second Questionnaire is PNRQ (refer Annexure 2) which is a 13 item tool, used to examine the risk associated with postnatal period. Score 5 for “Yes” and 0 for “No”. Sum all scores (yes/no and circled answers). The maximum score is 77; minimum is 10. There is no cutoff score at this stage; but a score above 24 with the presence of more that 2-3 risk factors at a significant level (score of 4 or 5) needs further enquiry as indicated by found psychosocial care needs.
The study was conducted for 6 months.
H0: There is no difference of postpartum depression among working and non-working mothers.
H1: There is a difference of postpartum depression among working and non-working mothers.
H0: There are no associated risk factors of postpartum depression among working and non-working mothers.
H1: There are associated risk factors of postpartum depression in working and non-working mothers.
Instrument was administered to those who gave written consent.
The primary investigator interviewed the 500 postpartum mothers (250 working and 250 working) after obtaining written consent. Two forms were filled by the investigators after asking the questions. Some demographic details were also included. The depression scores were calculated and were correlated with workplace problems. The data were qualitative and quantitative.
In this study mothers met the inclusion criteria if they: (1) had a baby within the previous 6 weeks to 12 months (2) are working women in any of the organization, (3) are nonworking mothers, those who are housewives. (4) Primigravida mothers, (5) free from any complication during pregnancy (6) are willing to participate in the study after obtaining written consent and are able to speak Urdu or English.
(1) Mothers who had delivered twins, have a stillbirth, or have delivered an infant with abnormalities, (2) Females who are not working, (3) Females who had postpartum period more than a year before and married females who had no children.
SPSS statistics version 2-0 was used for the data analyses. Mean and standard deviation was used for all continuous variables and frequency and percentages was used for all categorical variables.
A t-test was used to determine if there is a mean difference in working and nonworking mothers. A chi square test was used to determine whether there is an association of working and no working mothers with other variables. A pvalue of < 0.05 was used to determine level of significance.
Ethical consideration was taken care at the time of recruitment; permission was taken from working mothers who are interested in participating. Then written consent was taken from interested participants. Mothers provided an opportunity to ask questions and once they are satisfied with the explanations, they were requested to sign the informed consent. Data was collected after informed consent.
Overall 500 participants were selected for the study out of which 250 were non-working women and 250 were working women. Mean age of non-working mother group was 28.8±4.9 years. Regarding mother tongue of the participants', majority in non-working mother group were Urdu speaking, (58.4%). The majority of the participants were educated above matric 74.2%.
As far as the gestational age of the non-working women at the time of delivery of the baby is concerned, the majority were >37 weeks (69.2%). The weight of the baby at the time of delivery in this group was also standard i.e 2.5Kg or more (80.0%).
Moreover, mean age of working mother was 29.8±4.8years. Regarding mother tongue of the participants' majority belonged to Urdu speaking. Most of the participants were educated above matric.
In working women majority (97.2%) were employed in private sector. Income of the majority working women was between Rs. 15001-50,000.
Family structure also plays an important role. In non-working women, majority belonged to the extended family structure (55.6%) whereas in working women, nuclear family pattern was more (63.2%). However, it was not statistically significant for both the groups for the question whether they had planned for this pregnancy. Reply by majority of both the groups was positive (88.8% in nonworking women and 89.6% in working women). Family support was also positive in majority of both the groups (89.6% and 78.4% respectively). Similarly education status of the husbands of the participants was also above matric (86.8% and 78.8%respectively). Similarly majority of the husbands of non-working women and working women were also doing jobs in private sector (56.8% and 68% respectively). The income of the husbands of the nonworking women and working, women were also in the same range. Regarding husbands support in taking care of the child, majority of the non-working women replies yes (80.0%), however, it was just 50% of working women. The difference was found to be statistically significant (P<0.000). Similarly parents' in-laws and friends support in the care taking of the child was more in non-working women as compared to working women. This difference in both the group was statistically significant at P<0.000.The main issue of the study was to focus on the postnatal depression assessment. In order to achieve the purpose, Edinburgh postnatal depression scale and postnatal Risk Questionnaire (PNRQ) are used as instrument tools (Table 1).
Table 1. Comparison of mean EPDS and PNRQ between non-working and working women
According to Edinburgh postnatal depression scale, no depression was found in 202 participants of non-working women (80.8%) whereas in working women only, 89 participants reported no depression (35.6%) and this difference was found to be statistically significant at P<0.000.
Similarly, according to Postnatal Risk Questionnaire (PNRQ) score, <2 of the risk factor of postnatal was found in 221 non-working women (88.4%) and 157 working women (62.8%) whereas >2 of the risk factor of postnatal was found in 29 non-working women (11.6%) and 93 working women (37.2%). This difference was also found to be statistically significant at P<0.000 (Table 2).
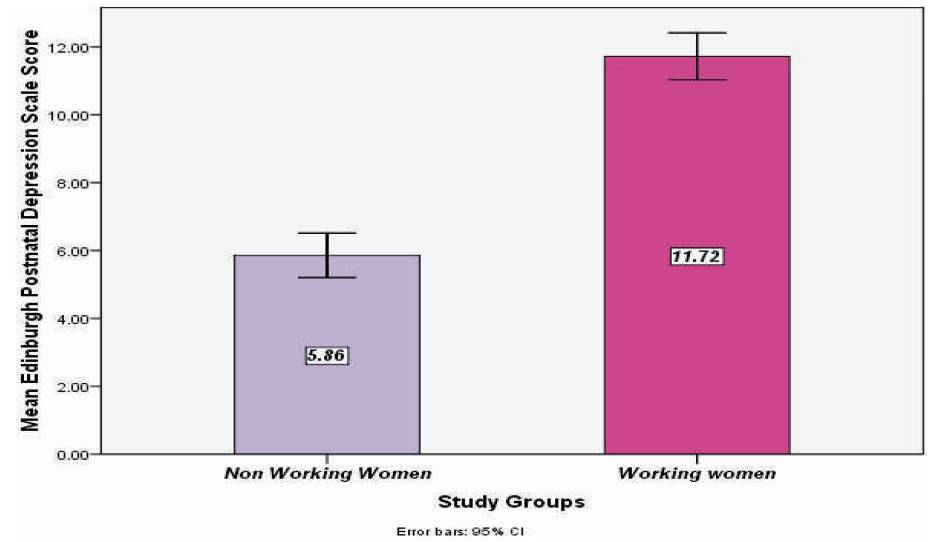
Figure 1. Postnatal depression scale (EPDS) in non- working women was 5.9 ± 5.3 whereas in working women it was 11.7 ± 5.6.
Stress is a multidimensional phenomenon and many studies indicate that working women have many types of stress in their life. According to World Bank report 2012, the share of women in Pakistani workforce was 28%. In a study (GK, P. & Arounassalame, B. (2014), the majority of the women 226/254 were in between the age of 20-30 years, with majority (192) educated intermediate, with only 54/254 being graduate. Husbands education was intermediate for 183/254. It is similar in this study results where mean age was 28.8±4.9 years in nonworking women and 29.8±4.8 years for working women. The majority of the participants of the study were educated above matric in both the groups' i.e 74.2% and 87.0%. Similarly, education status of the husbands of the participants in this study was also above matric (86.8% and 78.8%).
Figure 2 shows the Postnatal risk questionnaire (PNQR). The score was 15.5 ±9.5 in non-working women and 22.5 ± 10.5 in working women.
In this study, for 59.4% participants, family structure was extended family (joint family system). Similarly the pregnancy was planned in 89.2% of the participants. In a study conducted by GK, P. & Arounassalame, B. (2014) were the same result was shown as in that study, the majority 58.7% living in extended family setup and 79.9% had planned pregnancy. Postpartum depression remains changed in different areas and countries and work environment of women. In a study (Srinivasan, Nivetha, et al. 2015). Majority of the participants (65%) had scored 13 or higher on the EDDS scale reflecting high chance of depression. In a study (Adhikari, Harasankar 2012), the result showed that there were significant differences in degree of depression and anxiety of working mothers' group. In the study which was done on non-working women and working women to determine the level of postpartum depression the results showed that on Edinburg Depression Scale in non-working women was just 5.9 ± 5.3 where as in working women it was almost double i.e. 11.7 ± 5.6 [Figure 1]. It means that working women are also at high likelihood of depression.
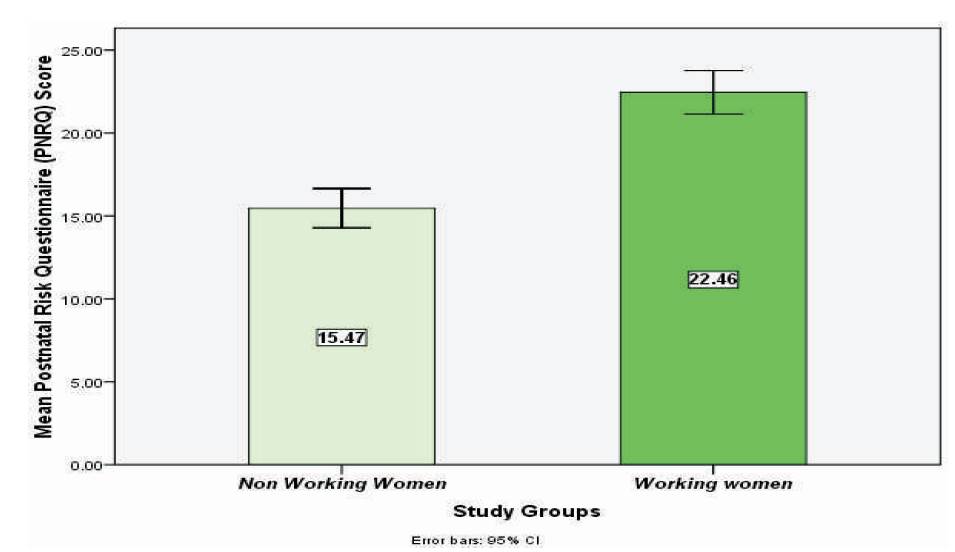
Figure 2. Postnatal risk questionnaire (PNQR) the score was 15.5 ±9.5 in non-working women and 22.5 ± 10.5 in working women
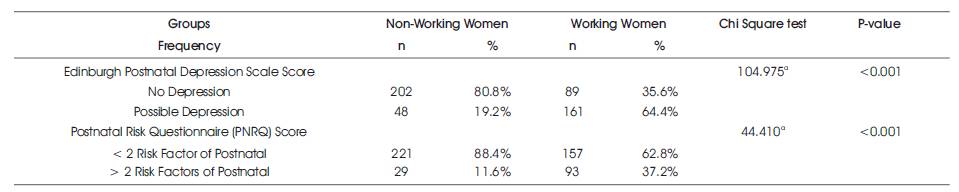
Table 2. Comparisons of frequency distribution of EPDS and PNRQ between non-working and working women
Different studies describe different risk factor of the postpartum depression. A study (Selix, Nancy W, et al. 2015) concludes that national policies are helpful for a better atmosphere for the working women and to reduce their risk of developing the postpartum depression. Similarly, different studies concluded that Type of marriage, recent stressful life event, dependence on husband, past history of psychiatric illness were significantly associated with PPD. In this study it was found that working women have almost the same risk factors, however they are at much lower level in the non-working women. Figures 3 and 4.
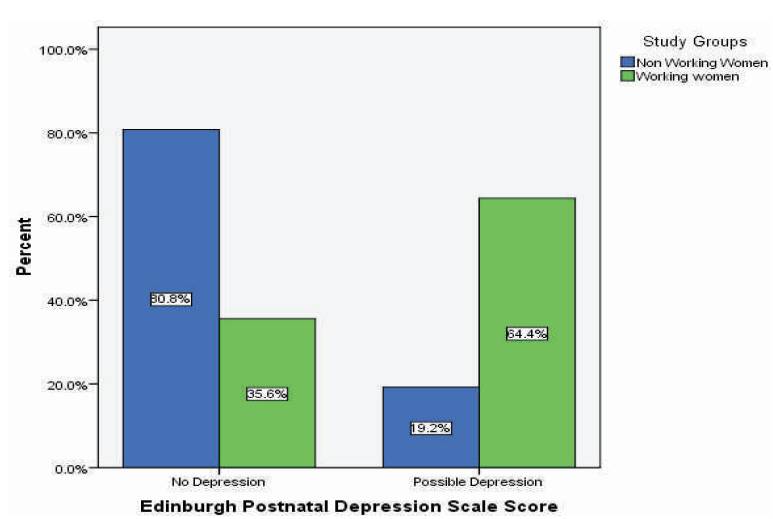
Figure 3. Comparative analysis of level of depression in working and non-working women and data revealed that according to postnatal depression scale (EPDS) working mothers have high level of depression rather than non-working.
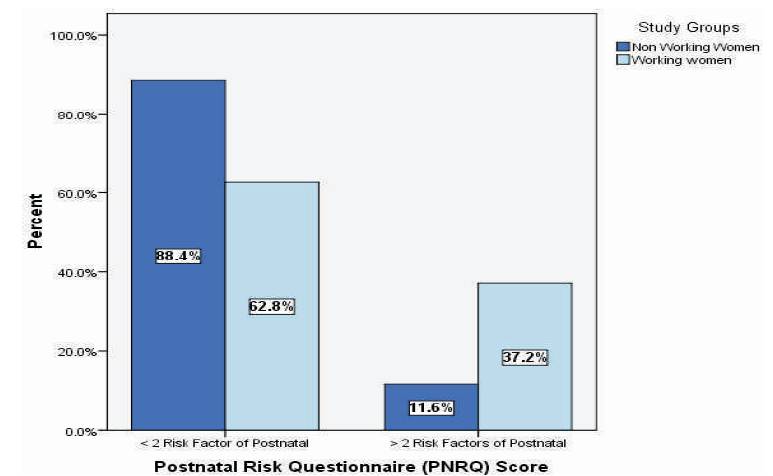
Figure 4. Postnatal Risk Questionnaire (PNRQ) score, <2 postnatal risk factors found in non-working mothers, whereas >2 risk factor of postnatal risk was found in working mothers. This difference was also found to be statistically significant.
Birth to a new life is, on one hand a pleasurable event in a mother's lifetime; on the other hand, it is a significant period when mother undergoes the transitional process from womanhood to motherhood. A significant difference was found in the rate of PPD measured from the birth of newborn within one year after delivery among working and non-working mothers. The study revealed that there is a high rate of depression that is of 64.4% in working mothers as compared to non-working that was 19.2% respectively due to various contributing factors. Pregnancy is a very crucial period for a woman and her family. The study findings showed that having Postpartum depression is a common factor and it could be reduced by the full support of the inlaws, husband's attention, and other family members and friends. Early detection of symptoms can facilitate timely treatment, and referral to appropriate health care providers in order to prevent from major depression.