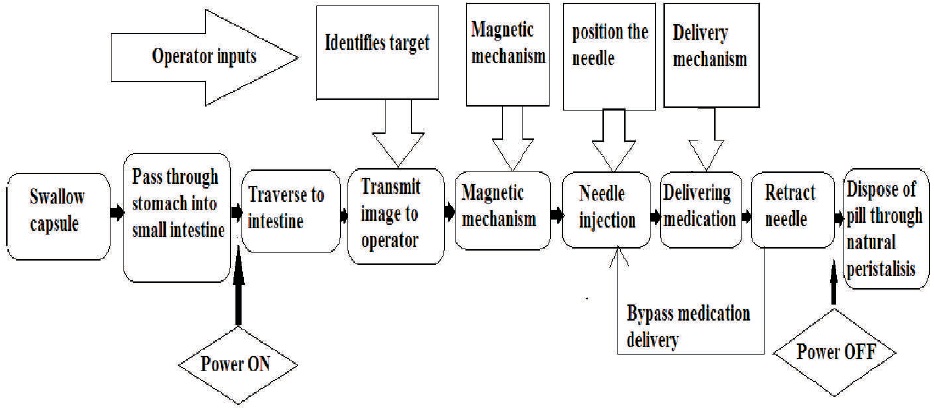
Figure 1. Block Diagram of Targeted Drug Delivery
This paper mainly describes a platform to achieve targeted drug delivery in the next-generation wireless capsule endoscopy. Targeted drug delivery helps in giving the medicine to the affected area only instead of giving it to the entire body. The major mechanism of the proposed system is the micro-positioning of the targeted medication with a level of 1 ml. This micro-positioning enables us to place the capsule in the required direction. The proposed micro-positioning mechanism allows a needle to be positioned within a 22.5° segment of a cylindrical capsule and be extendible up to 1.5mm outside the capsule body. The locomotion of the microrobot is achieved by magnetic mechanisms, which helps in holding the capsule as well as resist the peristaltic movement when necessary. The proposed infrastructure of the mechanism can be done using the combination of a single micro-motor with a volume of 200 mm3. An in-intensity evaluation of the mechanics is furnished and a top-level view of the requirements important to comprehend fashionable system integration is cited right here. This paper mainly aims to give the medication to the specified location. This will reduce the reaction of the drugs especially those drugs which are used for cancer treatment. Cancer treating drug when given through blood will reach all other organs before reaching the diseased tissue or part of the organ. Not only that, but it also helps to turn down the cost of drugs used for the cure. It is envisaged that the targeted drug delivery platform will empower a new breed of capsule microrobots for therapy in addition to diagnostics for pathologies such as ulcerative colitis and small intestinal Crohn's disease.
An endoscope is a device used to view the path of the Gastrointestinal Tract visually. It consists of a rigid or flexible tube, a light delivery system to illuminate the organ or object under inspection. The light source used is normally outside the body and the light is typically directed using an optical fiber system and a lens system transmitting the image from the objective lens to the viewer, typically a relay lens system in the case of rigid endoscopes or a bundle of fiber optics in the case of a fiberscope, an eyepiece, an additional channel to allow entry of medical instruments or manipulators. Surgical tools can also be inserted to the end of the endoscopic tube, which are handled at the other end of the tube (Wilding et al., 2000). They are used to investigate symptoms, such as symptoms in the digestive system including nausea, vomiting, abdominal pain, difficulty swallowing and gastrointestinal bleeding, and they are also used for confirmation of diagnosis, most commonly by performing a biopsy to check for conditions such as anemia, bleeding, inflammation, cancers of the digestive systems, giving treatments such as cauterization of a bleeding vessel, widening a narrow esophagus, clipping off a polyp or removing a foreign object. Speciality professional organizations that specialize in digestive problems advise that many patients with Barrett's esophagus are too frequently receiving endoscopies (Woo et al., 2010). Such societies suggest that patient with Barrett's esophagus and no cancer symptoms after two biopsies get biopsies as demonstrated and no more often than the recommended rate.
An Endoscopy is a basic methodology that permits a doctor to look inside human bodies using an instrument called an endoscope. A cutting tool can be attached to the end of the endoscope, and the apparatus can then be used to perform surgery.
Now after knowing an idea about what endoscopy is, let us move on to the next level of endoscopy that is Wireless Capsule Endoscopy (WCE). WCE is the same as an endoscope except that it does not have any fiber tube, instead it uses a single capsule to view the in body visually (Xiaona et al., 2005). They offer a feasible non-invasive way to detect the whole Gastro Intestinal (GI) tract and revolutionize the diagnosis technology. The patient doesn't need to bear all those pain; he/she just has to swallow the capsule which will do the exact thing. However, compared with wired endoscopies, the limited working time, the low frame rate, and the low image resolution limit the wider application. The advancement of this new technology is assessed in this paper, and the evolution tendencies are investigated to be high image resolution, high frame rate, and long working time. Shockingly, the power supply of capsule endoscope (CE) is the bottleneck. Wireless power transmission (WPT) is a promising answer for this issue, but is also a technical challenge. Active CE is another tendency and will be the next generation of the WCE. Nevertheless, it will not come true shortly, unless the practical locomotion mechanism of the active CE in the GI tract is accomplished. The locomotion mechanism is the other technical challenge, besides the challenge of WPT. This paper presents a platform for delivering a targeted dose of medication in a confined consistent cylindrical condition (Metzger et al., 2009). The platform comprises a magnetic mechanism and a needle positioning mechanism, which are integrated into a WCE. The magnetic mechanism is used to navigate the capsule and the needle positioning mechanism is used to place the needle in the desired direction. This integration gives increased functionality allowing the WCE to be used for targeted drug delivery in the GI tract. Targeted drug delivery means, giving medicine to that particular affected area.
There are several wireless capsule endoscopes (WCE) available for detecting and diagnosing pathologies of the gastrointestinal (GI) tract such as small intestinal Crohn's disease, obscure gastrointestinal bleeding (OGIB), and small intestinal tumors. The first endoscope was developed in 1806 by Philipp Bozzini in Mainz with his presentation of a "Lichtleiter" (light conductor) for the examinations of the canals and cavities of the human body. The utilization of electric light was a significant step in the improvement of endoscopy. In the beginning external lights are used, then later smaller bulbs became available making internal light possible, for example in a hysteroscope by Charles David in 1908. Hans Christian Jacobaeus has been given credit for early endoscopic investigations of the abdomen and the thorax with laparoscopy (1912) and thoracoscopy (1910). Laparoscopy was used in the diagnosis of liver and gallbladder sickness by Heinz Kalk during the 1930s. Hope reported in 1937 on the use of laparoscopy to diagnose ectopic pregnancy. In 1944, Raoul Palmer put his patients in the Trendelenburg position after gaseous distention of the abdomen and thus was able to reliably perform gynecologic laparoscopy. Georg Wolf (1873–1938) a Berlin manufacturer of rigid endoscopes, established in 1906, produced the Sussmann flexible gastroscope in 1911. Karl Storz started delivering instruments for ENT specialists in 1945. His goal was to develop instruments that would empower the practitioner to look inside the human body. Basil Hirschowitz and Larry Curtiss designed the first fiber optic endoscope in 1957. Before the 1950s, Harold Hopkins had planned a "fiberscope" comprising of a bundle of flexible glass fibers able to coherently transmit an image. This proved useful both medically and industrially, and subsequent research led to further enhancements in image quality. The elegant solution that Hopkins produced (in the late 1960s) was to occupy the air-spaces between the 'little lenses' with rods of glass. These fitted precisely in the endoscope's tube, making them self-aligning, and required no other support. This permitted the little lenses to be dispensed altogether. The rod-lenses were much easier to handle and used the maximum possible diameter available. In 1949, a Doctor working at the University of Tokyo Medical Center requested Olympus Optical Co., Ltd. (currently now Olympus Corporation) to develop a camera that could photograph and examine the interior of a patient's stomach. Olympus undertook this difficult challenge, and the historic development of gastrocameras started. After announcing the first WCE system in 2000, the Given Image Company released the first commercial WCE product system M2A in Yoqneam, Israel. The CE of the system is 11 mm in diameter and 26 mm long, which is small enough to be swallowed by the patient.
The name of M2A was changed to PillCam (implies Pill and Camera) later. In 2005, Given Imaging developed two distinct WCE systems: PillCam ESO specially for esophagus and PillCam SB specially for the small intestine. The CE is made out of 7 primary models including optical dome, short-focus lens, CMOS (Complementary Metal Oxide Semiconductor) image sensor, RF (Radio Frequency) transmitter, MCU (Micro Control Unit), LED (Light Emission Diode) lighting, and cell battery. PillCam COLON is another product of Given Imaging, which specially aims at visualization of the colon mucosa and identifying polyps. After FDA rejected the PillCam Colon application in the USA in 2008, Given Imaging developed the second generation PillCam COLON 2 and got a CE Mark in 2009 and was commercially available in Europe in 2010. The delivery methods employed by these devices prevent the direct targeting of specific pathogens such as tumors or ulcers as the medication is spread over a section of lumen due to the constant movement from peristalsis. Further, they have no means of stopping and holding their position.
Here the proposed unique features for endoscopy (GI tract diagnosis) that provide physicians with unprecedented imaging capabilities of the small bowel, including high resolution, a wider field of view, and enhanced depth of field. It supports early treatment of pre-malignant and early malignant lesions.
Conventional WCE has small geometry to permit them to go through the small digestive organs and explore the ileocolic valve without being an obstruction (Connor et al., 2009). Notwithstanding, the clinical need to focus on a specific area or feature within the GI tract for medication delivery or examination of the intestinal wall would require the WCE to stop.
The Gastrointestinal tract of the human body which starts from the mouth and ends to anus is a continuous channel through the body with orifices and specific motions for intake and output of external material. It consists of a series of organs with the billiard tract as a major side-branch. It should be mentioned here that the structure and function of the gastrointestinal tract differ among animals and humans according to the nutritional mechanism. The size of the gastrointestinal tract system depends on types of material passing through it in the long term. The wall of passage between the pharynx and the stomach tract has a laminated composite muscle structure, which is called the esophagus. Once swallowed, the WCE will pass through the elementary canal. The particular section of interest for diagnosis and treatment is the small intestines as this section is very difficult to access. The small digestive organs contain the duodenum, the jejunum, and the ileum. These three segments make up the longest part of the alimentary canal at 6.25 m. The duodenum is C-shaped and its mouth, the ileocolic valve, extends from the stomach giving this segment a degree of stability. The jejunum and the ileum are free to move; however, their natural state is collapsed. To process foodstuff, a liquid mixture called chyme, the small intestines use a a series of movement patterns. These patterns, segmentation and peristalsis cause the chyme to advance through the tract. Segmentation is the contraction of the duodenum to blend food. There are two processes involved: they are eccentric contractions and concentric contractions. The first creates almost no intraluminal pressure and the second can produce pressures as high as 20 mmHg. The frequency of the contractions is dependent on eating patterns, becoming stronger as chyme is being processed. Peristalsis is the process of moving chyme through the intestinal tract from the stomach to the colon by means of a series of muscle contractions acting in a wave design. The muscle contractions acts in two planes: circumferential and longitudinal. Miftah has built a mathematical model to describe the dynamics the electro mechanical wave phenomenon of a segment of the gut. They reported that the active force of contraction in the longitudinal direction should have amplitude of 26.9 g/cm and amplitude of 17.2 g/cm in the circumferential direction. For a conventional WCE with measurements of 11.0 mm diameter × 25.0 mm long, the circumferential and longitudinal amplitudes convert into 421.8 and 911.9 mN, respectively.
There are three methods employed for halting the progress of a WCE by enabling it to resist the natural movement from peristalsis. One uses micro actuator mechanisms embedded within the capsule, such as paddling-based micro robot developed by Park et al. (2007). The second approach is holding mechanism to resist peristaltic movement employed and the third approach applies a stimulus to GI tract to inhibit peristalsis. There have been several systems employed by researchers to stop the microrobot, such as insufflation of the tract using balloons or expanding legs. However, these systems exhibit limitations. In the case of the expanding legs, they are driven by a lead screw, which is powered by a micro motor. The lead screw and the micromotor are axially aligned with the microrobot. This configuration requires a substantial amount of space and presents problems of force translation through the legs due to the lever effect.
To overcome the peristalsis, a magnetic mechanism compact enough to fit within the microrobot is required. This methodology misuses outer attractive fields to control the position of the capsule. This system looks to modify existing WCE with the addition of a magnetic shell (Cave et al., 2008). The shell can be used to guide the WCE by means of an outside attractive field; however, this system requires large equipment to perform the procedure and there is also an increase in the diameter of the WCE.
The overall geometry of the micro-robotic system will be greatly influenced by the limitations imposed by swallowing and on its ability to navigate natural obstacles such as the ileocolic valve without becoming an obstruction. A patient's ability to swallow a required volume will change from individual to individual; accordingly, a standard volume must be chosen which will be appropriate for the majority of patients. Research carried out by Connor et al. shows that a volume of 3.0 cm can be gulped. This 3 maximum target volume will be required to house all the components necessary to perform targeted therapy and micro scale diagnosis (Carpi et al., 2007).
The main sequence of events required to perform a procedure to deliver treatment to the GI tract can be seen in Figure 1. The procedure starts with the patient ingesting the WCE.
Figure 1. Block Diagram of Targeted Drug Delivery
When the capsule passes through the stomach and enters the small intestines, it can start to transmit images to the operator using a RF interface. The real time images and sensor data will be displayed on an external PC. The operator will use the data to identify defined target site. When the objective site has been reached, the operator will use the magnetic mechanism for rotating and positioning of the micro robot. The operator can now rotate the capsule into any one of desired positions. The position will be based on observational data received through the camera. The needle can now be advanced into the GI tract wall and the medication is released.
The targeting mechanism is designed such that it gives the operator the ability to reposition the needle before the medication is delivered (Epstein, 2009). Finally, the capsule will be dispelled through the anus by natural peristalsis movement.
At the time an external object passes through the human's mouth, muscles in the GI tract start to move sinusoidally (peristalsis wave) and helps an object to pass the esophagus to the stomach. This is the resistance force applied to the capsule robot during its operation that the magnetic control system is going to produce a locomotive force opposite to peristalsis wave. Regarding this fact, the capsule robot can stay at a specific point to release the drug at that point. A similar method in medical applications like chemotherapy in esophagus cancer is done by delivering the drug through the blood (Forgione, 2009). This destructive drug can then damage the targeted cells. On the other hand, drug delivery should be performed for a long time. These two major aims can be achieved by keeping the capsule at the desired point and release the drug for a long time at that point.
Micro-robot propulsion can use a spiral-shaped exterior of the capsule which directs surrounding fluid when the robot rotates, pushing the capsule forward (Toennies et al., 2010). A magnetic film deposited on the capsule rotates the robot when a rotating external magnetic field is applied, allowing the motion of the robot to be controlled. The frequency of rotation is directly related to the speed of the robot. Figure 2 pictures the magnetic propulsion model.
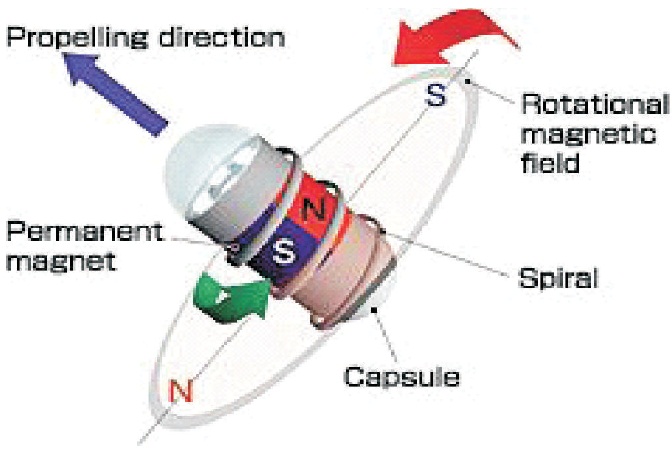
Figure 2. Magnetic Propulsion Model
The proposed method is for determining position and orientation, using X-ray radiation, of an endoscopic capsule, driven by an external magnetic field. In this case, the determination of the position and orientation of the capsule is helpful to generate the correct magnetic field for capsule navigation. In this invention, an X-ray was used for both the exact positioning and elimination of interfering with the signals of position tracking and magnetic field. This proposal includes an endoscopic capsule, a navigation device for generating the magnetic field, and an X-ray machine for recording radiation images (Gray, 2005).
When treating conditions such as small cell cancer, chemotherapy is usually administered intravenously or through pills. These methods do not specifically target the cancerous cells (Valdastri et al., 2009), damaging healthy cells and reducing the effectiveness of the treatment. Delivering drugs to specific sites can improve the effectiveness of treatment and reduce the adverse effects of the chemicals. Capsule robots could deliver medication to specific targets. This would be a further improvement over many existing capsule robots which merely observe the affected areas. Periodic drug release for a longer time is another goal of the drug delivery system of capsule robot. The present paper has been proposed to provide wireless control with the drug delivery system.
The drug delivery system functions by storing medication in stretched balloons and upon triggering expels the drug through a needle by allowing the balloons to contract. Designs operating on a similar (Goldfarb et al., 2005) and principle use microvalves. A search was conducted for a suitable commercially available micro value however no such device was found. As an alternative a design was envisioned in which a piston acts to hold the drugs in the balloon. A solenoid would then move the piston to release the drugs as the balloon contracted. Then the drug will be injected into the targeted tissue into which the needle is inserted. The outer cylinder would be wrapped in wire. When the wire conducts current, the piston would be moved by the magnetic field generated by the wire. This design was determined to be infeasible because the number of turns of wire would be too high. It was decided that the use of a commercial solenoid would be a better choice (Miftahof, 2005).
To avoid the limitation of solenoid, shape memory alloy is recommended for drug delivery. In this iteration of drug delivery, the plastic tube of the pressurized drug is located inside the capsule robot. The SMA is located at the position that touches this plastic reservoir with minimum force applying to this reservoir. SMA is connected to the internal circuit which can apply voltage to its both ends and change its length. Therefore, it makes a hole in pressurized tubes and the drug will be released there. The goal for drug delivery in our system is to have a wireless actuation of releasing the drug the same as a wireless magnetic control system.
The designed macro robot that depicts a wireless capsule endoscopy with targeted drug delivery for demo purposes. The block diagram in Figure 3 shows the components used and how they have been integrated to make the model work. Figure 4 shows the side view and front view of the macro robot. The macro robot is designed to move inside a PVC pipe by using 6 wheels which have been rotated by 6 motors. The PVC pipe is the model used as a substitute for the human gastrointestinal tract.
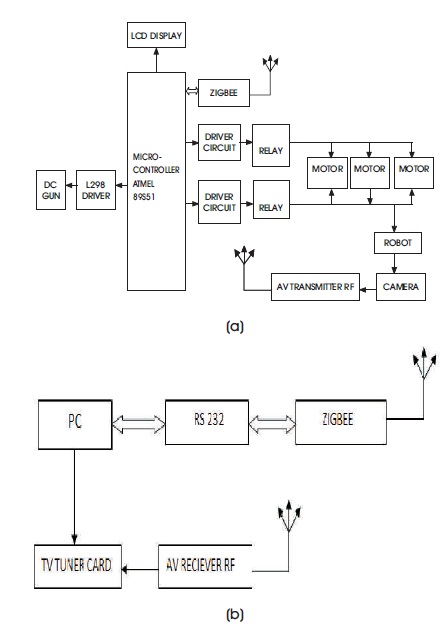
Figure 3. Block Diagram of Designed Macro Robot (a) Capsule Part (b) Control Part
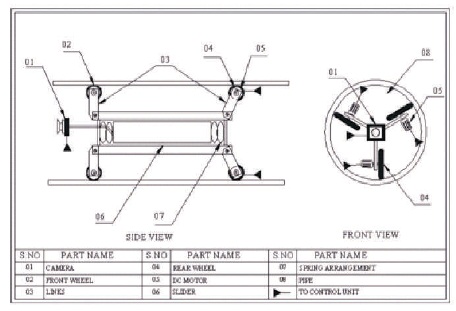
Figure 4. A Side View and Front View of the Macro Robot
This model consists of two parts.1) Capsule robot model 2) External control model. Capsule robot will be moving inside the PVC pipe and the robot is controlled from the designed control model placed external to the PVC pipe (Park et al., 2007). This is like controlling the capsule inside the GI tract from outside the patient's body using the wireless RF control mechanism.
Micro controller AT89S51 used is the heart of the capsule robot. It controls all other entities used in the design of the capsule robot. Other entities include CMOS image sensor for capturing video of the Gastro-Intestinal tract, LEDs for illumination so that pictures can be captured clearly, an AV transmitter module for the transmission of captured video to the external control unit, a DC motor for actuating needle positioning and targeted drug delivery, separate 6 DC motors for the forward/reverse locomotion of the robot inside the PVC pipe, a 16x2 LCD module to display “Wireless Capsule Endoscopy”, a Zigbee receiver module for the reception of control signals from the external control unit wirelessly. The DC motor used for the targeted drug delivery mechanism is interfaced with AT89S51 using the L298 H bridge driver. The 6 DC motors for locomotion are interfaced to the micro controller using relay circuits (Rao et al., 2009).
In the external control unit, a personal computer is the heart as it has a micro controller (artificial brain) and provides a user interface where the user has the human brain(Woods & Constandinou, 2011). So PC, which is under the user's control, controls the other entities used in the design of the control unit. Other entities include a Zigbee transmitter module for the transmission of controls as desired by the user to the Zigbee receiver module interfaced to the micro controller in the capsule robot, the receiver module for the reception of captured video of GI tract sent from the capsule robot (Swain et al., 2004). The ZigBee module is interfaced with the PC through RS-232 cable and the AV receiver module is connected to the PC through a TV tuner card. A TV tuner card is a television tuner that allows a computer to receive television signals. Most TV tuners also function as video capture cards, allowing them to record television programs onto a hard disk.
The circuit in Figure 5 is intended to control the motor in the forward and reverse direction. It consists of two relays named as relay1, relay 2. The relay ON and OFF is controlled by the pair of switching transistors. A Relay is nothing but a electromagnetic switching device which comprises of three pins. They are Common, Normally Close (NC), and Normally Open (NO). The common pin of two relays is associated with the positive and negative terminal of the motor through the snubber circuit respectively. The relays are connected in the collector terminal of the transistors Q2 and Q4.
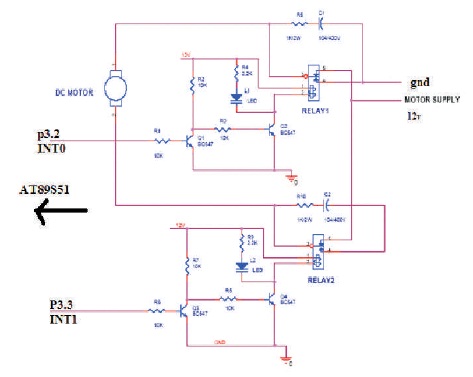
Figure 5. DC Motor Forward Reverses Control
When high pulse signal is given to either base of the Q1 or Q3 transistors, the transistor is conducting and shorts the collector and emitter terminal, and zero signals is given to the base of the Q2 or Q4 transistor. So the relay is turned OFF state.
When the low pulse is given to either base of transistor Q1 or Q3, the transistor is turned OFF. Presently 12 V is given to the base of Q2 or Q4 transistor so the transistor conducts and relay is turned ON. The NO and NC pins of two relays are interconnected so only one relay can be operated at a time.
The series combination of resistor and capacitor is called a snubber circuit. When the relay is turned ON and turned OFF continuously, the back EMF may fault the relays. So the back EMF is grounded through the snubber circuit.
Table 1 shows the working of the DC motor for locomotion.
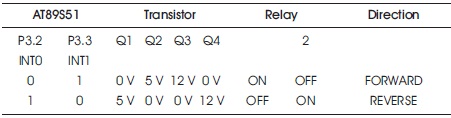
Table 1. Working of DC Motor for Locomotion
In the case of DC motor forward reverse control for needle mechanism shown in Figure 6, DC motor is interfaced with the AT89S51 using L298 H-bridge driver. The working of the DC motor for needle mechanism is shown in Table 2.
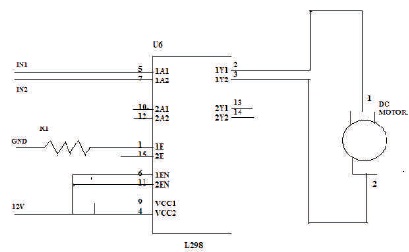
Figure 6. Single DC Motor Forward Reverses Control
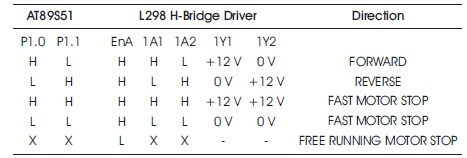
Table 2. Working of Single DC Motor for Targeted Drug Delivery
In the case of wireless Zigbee communication, Zigbee transmitter module is connected to the serial port of personal computer through a MAX232 IC and the ZigBee transmitter module is connected to the microcontroller directly as both are TTL compatible devices. Table 3 shows the working of the Zigbee receiver connected to micro controller AT89S51 directly. Table 4 shows the working of the Zigbee transmitter interfaced to the serial port of personal computer through a MAX232 IC. Figure 7 shows the interfacing circuit of the Zigbee transmitter to the serial port of a personal computer.
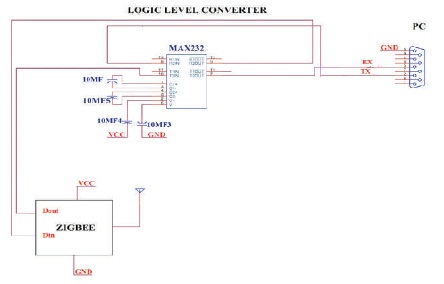
Figure 7. Interfacing Circuit of Zigbee Transmitter to a Personal Computer
The data transmitted from PC through the serial port will be in analog form. That is PC can receive and transmit data only in analog form when the serial port is used. But Zigbee module can accept and give back only transistor to transistor logic (TTL) data. So in order to convert the analog data from the serial port of PC to TTL data as the Zigbee module can accept, MAX232 IC is used. MAX232 IC can convert serial data to TTL and vice versa.
The gastrointestinal tract is home to some of the most deadly human diseases. Worsening the problem is the difficulty of accessing it for diagnosis or intervention and the attending patient discomfort. In traditional drug delivery system such as oral ingestion or intravascular injection, the medication is distributed throughout the body through the systemic blood circulation. For most therapeutic agents, only a small portion of the medication reaches the organ to be influenced.
Wireless capsule endoscopy thus offers an appealing alternative to traditional flexible scope-based endoscopy. Targeted drug delivery seeks to concentrate the medication in the tissues of interest while reducing the relative concentration of the medication in the remaining tissues. For instance, by avoiding the host's defense mechanisms and inhibiting non-specific distribution in the liver and spleen, a system can reach the intended site of action in higher concentrations. Targeted delivery is believed to improve efficiency while reducing the side effects.
The magnetic propulsion system helps the doctor with effective access to the entire GI tract. It also helps to hold the capsule for a long time near the tissue where the drug has to be delivered. A wireless power transmission system helps to prevent the mission failure due to the short life span of the battery. Moreover, we have described our macro robot depicting the microrobot in this paper.
One of the challenging applications in wireless endoscopy is a micro biopsy. The objective of this application is to acquire body tissue or a fluid sample at a desired location along the GI Tract. This sample is retrieved after the capsule is removed from the body for examination. Two mechanisms have been proposed. Mucosal biopsies using a spring-loaded Crosby capsule type device guided by real-time imaging capability. Radio frequency controlled remote manipulation or a rotational micro biopsy device consisting of a trigger with a paraffin block and a rotational tissue-cutting razor. Another mechanism has been proposed to operate sequentially so that tissue sampling, sealing and fixing are achieved in single operation.