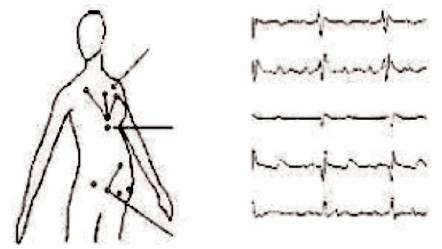
Figure 1. Lead Locations of ECG Signal Measurement in a Pregnant Woman
The electrocardiogram (ECG) signal is a graphical recording of the electrical potentials generated in association with heart activity, which is one of the many important physiological signals commonly used in clinical practice. The wellbeing and status of a fetus can be accessed from a fetal ECG signal. Detecting and analysing the fetal ECG is the primary objective of electronic fetal monitoring. This paper presents a method to separate fetal ECG signals from the maternal abdomen. The method is general and is able to separate the fetal ECG signals using any number of recording electrodes, including the difficult case of single channel. This approach is based on some simple mathematical model using convolution matrix and with the help of maternal ECG, the fetal ECG signals can be extracted from the maternal abdomen. Further, the fetal ECG signals are passed through wavelets and adaptive filter to reduce the noise in the fetal ECG. The results show that the proposed method has a promising performance.
The electrocardiographic (ECG) recording of a pregnant woman reflects the activity of the hearts of both mother and fetus [1]. This ECG is commonly measured at two locations namely chest and abdomen as shown in Figure 1. One typical electrode placement configuration is to measure five abdominal and three thoracic channel recordings [4]. The thoracic channel recordings contain the primarily maternal ECG signals. In contrast, the abdominal channel recordings are composite ECG signals that consist of both maternal ECG and Fetal ECG (FECG) signals. FECG signals are generally much weaker than maternal ECG signals while the fetal heart rate is usually higher than the maternal heart rate [6]. There are numerous reasons for changes in fetal heart rate. Most of these are because of normal adaptation by fetus to change in its environment such as normal alterations in fetal activity, placental blood flow, hypoxia, external stimuli, increase in temperature, and drugs.
Figure 1. Lead Locations of ECG Signal Measurement in a Pregnant Woman
The synchronization between the maternal and fetal heart rates were studied and it was not able to unconditionally conclude that fetal-maternal heart rate synchronization exists [7]. However, there was evidence in suggesting that occasional coupling occurs between fetal and maternal cardiac systems as shown in Figures 2 and 3. Moreover, there was a reason to expect the interaction between the maternal and fetal cardiac systems under some favourable conditions based on some studies [8].
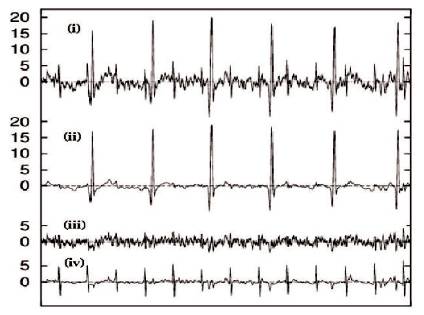
Figure 2. From Top: (i) Mixture of Maternal and Fetal ECG, (ii) Maternal ECG only (iii) Noise (iv) Fetal ECG
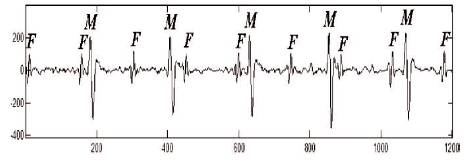
Figure 3. Abdominal ECG Recording, F: Fetal Influence, M: Maternal Influence
The electrocardiogram signal from the mother is analysed, and the mother’s heart rate for this signal is approximately 80 beats per minute, and the peak voltage of the signal is 35 millivolts, whereas electrocardiogram for fetus has the heart rate of 138 beats per minute and a peak voltage of 18.5 millivolts. The heart of a fetus beats noticeably faster than that of its mother, with rates ranging from 130 to 160 beats per minute. The amplitude of the FECG is also much weaker than that of the maternal electrocardiogram. The measured FECG signal is as shown in Figures 2 and 3. The abdomen of the mother is usually dominated by the maternal heart beat signal that propagates from the chest cavity to the abdomen [1] .
The recording of FECG is a simple and non-invasive method for monitoring the electrical activity of the fetal heart [4]. Like the standard ECG, which reflects cardiac and metabolic activity, FECG is potentially a sensitive indicator of fetal health state. A common situation in ECG signal acquisition is that the presence of noise, deteriorates the signal’s quality by decreasing the Signalto- Noise Ratio (SNR). The sources of interference when acquiring the abdominal signals are the maternal ECG, the myographic noise, the power line interference, the fluctuation of the baseline and factors related to the gestation week [2]. More specifically, the maternal influence in the composite signal has two main characteristics.
Moreover, the abdominal FECG signal is characterized by a poor SNR, while its shape depends on the position of the electrodes, as well as on the gestational week. The fact is that there is no standard electrode positioning for optimizing acquisition that makes the problem of automated Fetal Heart Rate extraction (FHR) more complex [1,8].
There are a variety of methods that exists for Electronic Fetal Monitoring (EFM). The two main non-invasive methods used in fetal monitoring are FECG and Fetal Magneto Cardio Graph (FMCG) [11]. Both methods can provide the fetal heart rate information with true beat-tobeat accuracy. Furthermore, morphological analysis can be performed as both FECG and FMCG which has the potential to provide a FECG [7].
Most recent studies indicate that a clinically useable fetal heart rate trace can be extracted for at least 60% of the recording time for long-term (8 to 24 hours) [1] recording from late gestation mothers. Another disadvantage of the fetal ECG is that around 28th to 32nd week of gestation, the amplitude of the FECG is markedly attenuated due to the electrically insulating effect of the vernix caseosa covering the fetus and the existence of preferred conduction pathways between the fetal heart and maternal abdomen around this time [9].
This method is divided into two parts.
For the extraction of FECG from abdominal ECG with the help of maternal ECG [2, 3], a simple convolution matrix is used as shown in Figure 4.
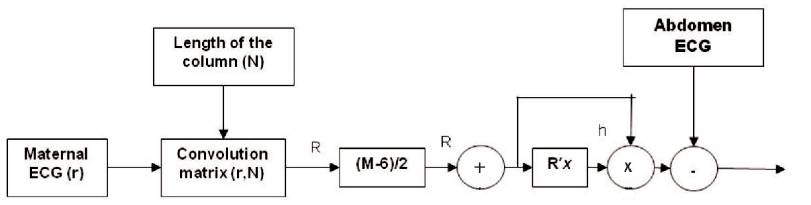
Figure 4. Block Diagram to Extract FECG
The extracted FECG signals are shown in Figure 5.
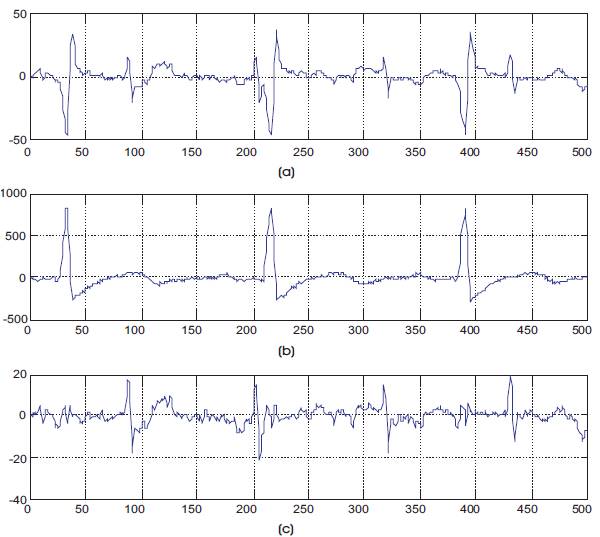
Figure 5 (a) Mixture of Maternal and Fetal ECG, (b) Maternal ECG Only, (c) Extracted Fetal ECG
The extracted output is subjected to denoise the FECG signal to extract the better signal for analysis. The proposed methods for denoising FECG signals in this paper are:
The wavelet denoising approach is based on the assumption that random errors in a signal are present over all the coefficients while deterministic changes get captured in a small number of relatively large coefficients [10]. As a result, a nonlinear thresholding (shrinking) function in the wavelet domain will tend to keep a few larger coefficients representing the underlying signal, while the noise coefficients will tend to reduce to zero. Practically, the wavelet denoising method consists of applying the discrete wavelet transform to the original noisy data, thresholding the detail coefficients, and then inverse transforming the thresholded coefficients to obtain the time-domain denoised data [9]. It should be noted that the performance of the wavelet denoising depends on the choice of the thresholding rule, the type of wavelet, the maximum depth of wavelet decomposition and the initial SNR.
Wavelet denoising procedure is as follows.
The wavelet denoising signal after extraction is shown in Figure 6.
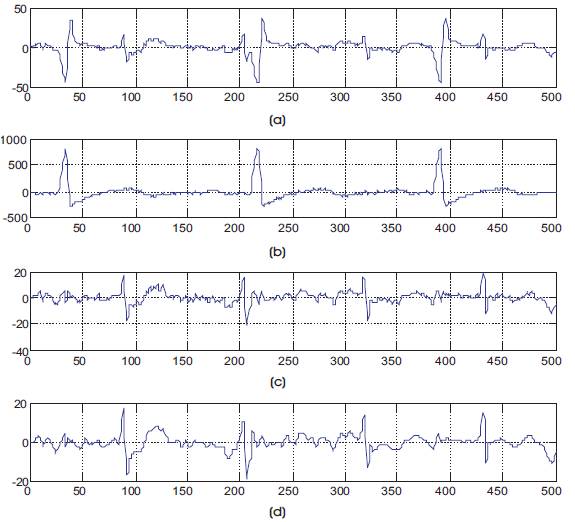
Figure 6. (a) Mixture of Maternal and Fetal ECG, (b) Maternal ECG Only (c) Fetal ECG, (d) Fetal ECG Signal After Wavelet Denoising
In order to use the LMS algorithm, we must first determine a filter order and then a good step-size [5]. This can be done by trail-and-error, or by finding the autocorrelation of the reference signal and the cross-correlation between the reference and primary signals. We know the filter order need not be larger than 60, whereas increasing the filter order did not degrade the performance of the optimal filter, rather it degrades the performance of LMS [5] . This is because of the larger filter order, the larger will be the eigenvalue spread among the autocorrelation matrix of the reference signal. Increasing the eigenvalue spread, decreases the rate of convergence of LMS to the optimal solution [5]. This occurs because the maximum step- size for convergence is related to the maximum eigenvalue, but the rate of convergence is proportional to the stepsize and the minimum eigenvalue, is shown in the Equation (1).
where T is the step-size, λmin is the minimum eigenvalue, and τ is the overall time-constant (which is inversely related to the convergence rate).
As a compromise, authors chose M = 20 for the order of the filter. If the rule of thumb, T = 0.2/λmax , then the theoretical convergence time constant for the LMS rule is given by Equation (2) which gives the time constant for the convergence of the slowest converging weight.

The adaptive denoising signal after extraction is shown in Figure 8.
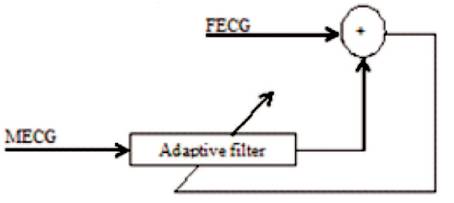
Figure 7. Adaptive Noise Canceller
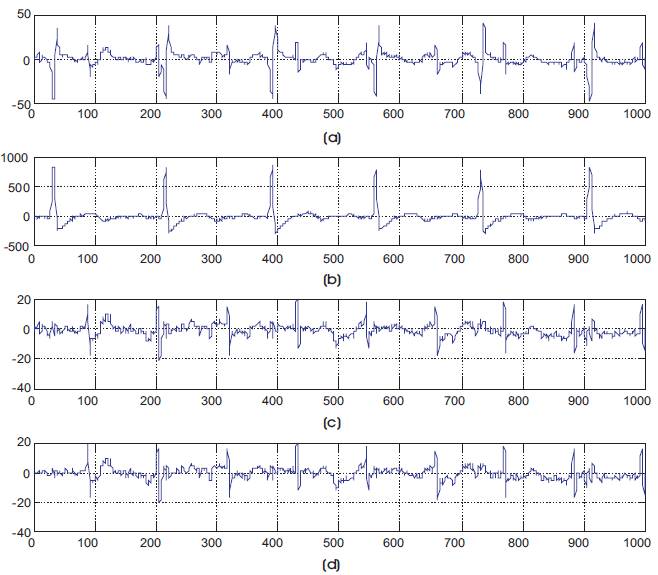
Figure 8 (a) Mixture of Maternal and Fetal ECG, (b) Maternal ECG Only, (c) Fetal ECG (d) Fetal ECG Signal After Adaptive lms Denoising.
In this method, the extracted FECG signal is passed through Db3 wavelet. The procedure has been explained earlier.
After extraction of the signal from the wavelet, this signal is passed through adaptive LMS. In order to use the LMS algorithm, the authors must first determine a filter order and then a good step-size [5]. This can be done by trailand- error, or by finding the autocorrelation of the reference signal and the cross-correlation between the reference and primary signals. The remaining steps follow same as in the Adaptive LMS Denoising Method. The output of both the wavelet and adaptive filters are shown in Figure 9.
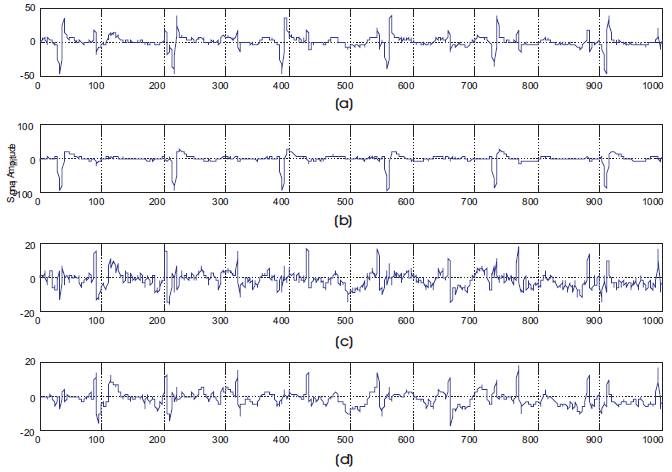
Figure 9 (a) Mixture of Maternal and Fetal ECG, (b) Maternal ECG Only, (c) Fetal ECG (d) Fetal ECG Signal After Adaptive + Wavelet Denoising
The extracted FECG signals from the abdominal and maternal recorded signal are taken from the database. Then wavelet and adaptive filters are used to suppress the harmonics of the fundamental frequency of the FECG signal as shown in Figure 7.
The signals are taken from the database to check the capability of the method in detecting the FECG signal. The obtained results indicate that accurate FECG can be detected using maternal ECG signals recorded from the mother's abdomen. The data used in this work is obtained from physionet.org and Sista/Daisy. The calculation is made for 55 samples and the sensitivity is found to be 98.18% as shown in Table 1 [2].
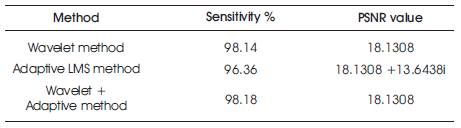
Table 1. Performance of FECG Extraction
The performance of the proposed methods was evaluated based on their sensitivity and it has been given by [2, 3],

The True Positive (TP) is the number of matched FECG i.e., correctly detected FECG, False Negative (FN) is missed detections i.e., number of events that were not detected by the approach.
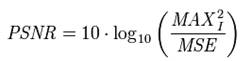
The Peak Signal-to-Noise Ratio, often abbreviated PSNR, is the ratio between the maximum possible power of a signal and the power of corrupting noise that affects the fidelity of its representation. Because many signals have a very wide dynamic range, PSNR is usually expressed in terms of the logarithmic decibel scale.
It is most easily defined via the Mean Squared Error (MSE) which for two m×n signals, I and K where one of the signal is considered as noisy approximation of the other is defined as:

The PSNR is defined as:
The wavelet and adaptive LMS noise canceller has been used to remove the noise from the extracted FECG. The Cardiac Signal Analysis has been implemented in MATLAB7.10 software. There are some more denosing techniques that are available which can used to remove the noise caused by the abdomen and mother ECG. This may give a better analysis on the Fetal signal.